A choking rescue case is not product proof. It is a readiness test. The useful questions are who saw the obstruction first, how fast first-line rescue began, whether 911 could be called without leaving the person, and whether second-line airway backup was reachable after first-line care failed.
For a household checklist, see Fitiger's child and home choking safety readiness plan.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
Public rescue stories often arrive as emotional headlines. A baby starts choking. A restaurant guest cannot breathe. A dining-room worker notices a resident in trouble. Someone moves fast, and the story ends with relief.
That version is easy to share. It does not give schools, child care centers, restaurants, assisted-living facilities, and families enough to improve their own response.
Those details turn a rescue story into an airway readiness audit. The lesson is not hero worship. The lesson is room design under pressure.

An infant choking rescue is useful because it shows how little time the first adult has to interpret the scene. A frantic family member, a choking baby, and responders moving before the setting looks organized: that is the part every daycare, preschool, and family should study.
For infants under 1 year old, the standard response is not a smaller version of the adult sequence. Infant choking response uses back blows and chest thrusts. Abdominal thrusts are not used for infants. Device-first thinking does not belong at the front of the sequence.
The practical lesson is simple: infant choking readiness is built before the snack, not during the panic.
If a child care worker has to remember the infant sequence for the first time while a baby is already silent, the system is late. If a second staff member does not know who calls 911, the system slows again.
Daycare and home readiness should cover the basics before an emergency starts.
A case can be inspiring. A drill changes the next response.
A restaurant choking self-rescue account teaches a different lesson. In public dining spaces, the perfect helper may not be there.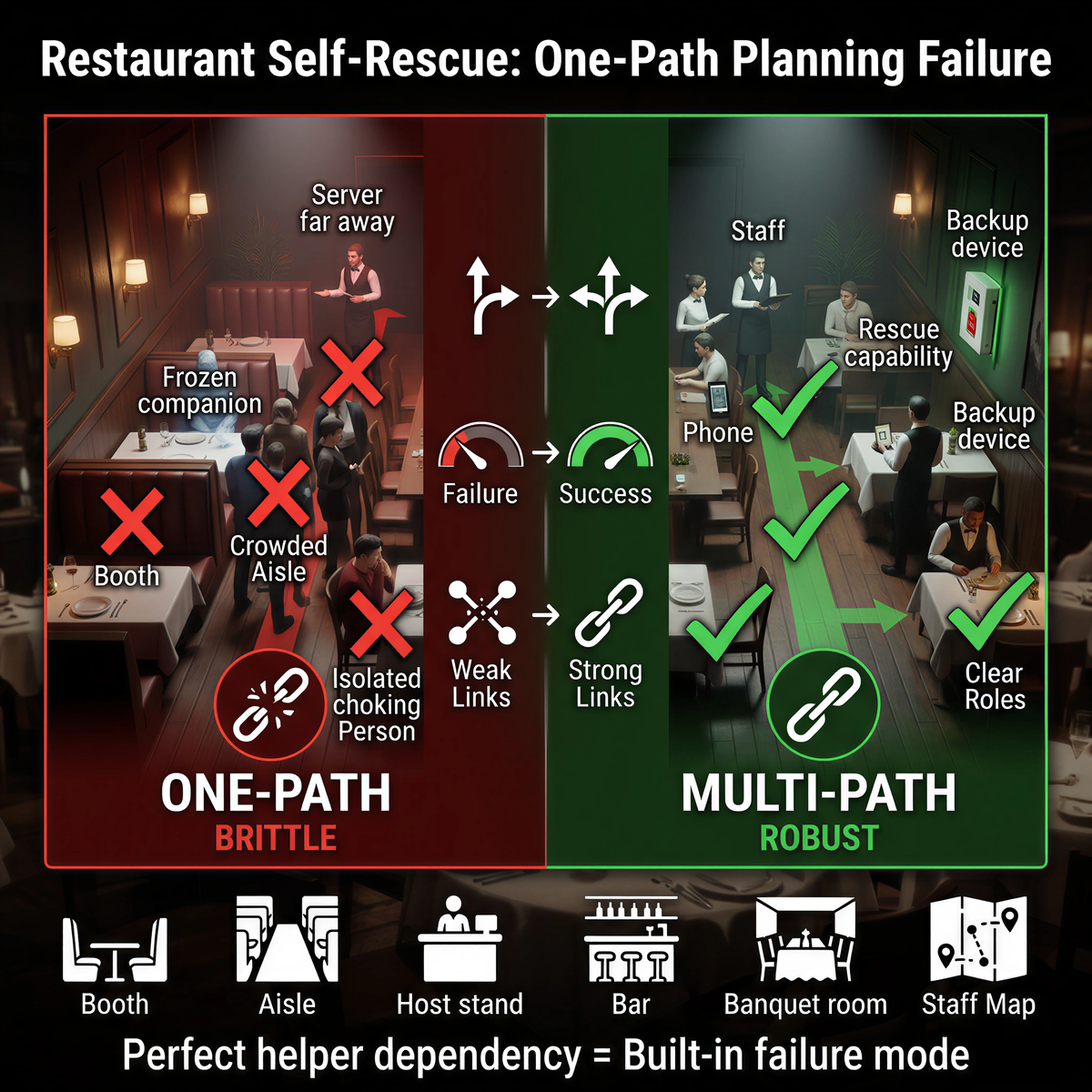
A server may be two tables away. A companion may freeze. A booth may make positioning awkward. A crowded aisle may block access. A person choking alone at a table may have only seconds to create a working plan.
This does not reverse the order of care. First-line choking rescue still comes first when a responder is available. 911 still needs to be activated. CPR readiness still matters.
The point is brittleness. If the entire response model depends on one physically ideal helper standing in the right place, the plan has a built-in failure mode.
Second-line airway response exists for that kind of failure point. A suction anti-choking device, when FDA-authorized and used within its instructions, belongs after unsuccessful basic life support choking protocol in a complete airway obstruction emergency. It is not the first reach. It is the backup path when the first path did not clear the airway.
Restaurants should not start with product storage. They should start with the booth, aisle, host stand, bar, banquet room, and staff role map.
In assisted living, memory care, and senior dining rooms, the first effective responder may not be the nurse down the hall. It may be a dining aide, activity assistant, family visitor, student worker, or whoever is already near the table when the resident stops moving air.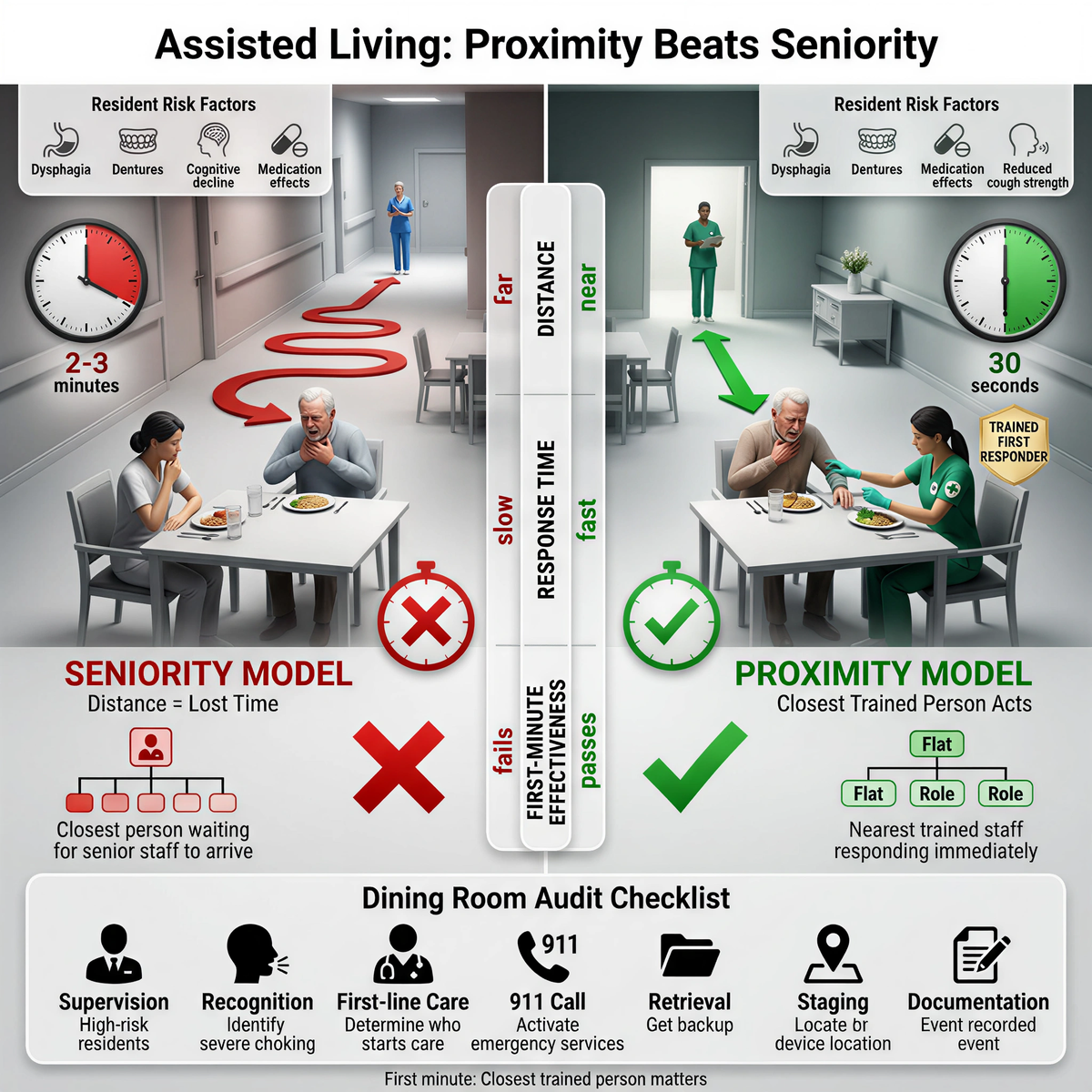
That reality matters because older adults can carry layered choking risk: dysphagia, fatigue, dentures, cognitive decline, medication effects, reduced cough strength, and slow recognition. A resident may cough once, reach for water, and then go quiet.
The staff member at the table may be the only person close enough to compress the timeline.
A care facility that writes a polished emergency policy but leaves the first witness unsure has not built a rescue system. It has built a document.
For nursing homes and assisted-living facilities, the better audit starts with the dining room.
Proximity beats seniority in the first minute. The closest trained person matters.
Schools and childcare settings often have written emergency procedures. The weak point is usually not the policy. It is the first witness.
A cafeteria monitor may be the first adult close enough to see the student’s face change. A substitute teacher may be supervising snack time. A coach may be outside on a field. A bus aide may be the only adult close to a student with a feeding or swallowing history.
The rescue case should become a drill script, not a story pinned to a bulletin board.
Run the scene from the actual choke-risk locations: cafeteria, classroom snack table, playground bench, bus seat, after-school room, and sports sideline. Measure recognition, first-line action, 911 delegation, route to backup resources, and EMS handoff.
A school that only drills from the nurse’s office is testing the wrong room.
Rescue cases are useful, but they can be misused.
The FDA’s QXN framework keeps the boundary narrow: suction anti-choking devices are second-line treatment for complete airway obstruction after unsuccessful BLS choking protocol. That boundary protects the response sequence from becoming a sales claim.
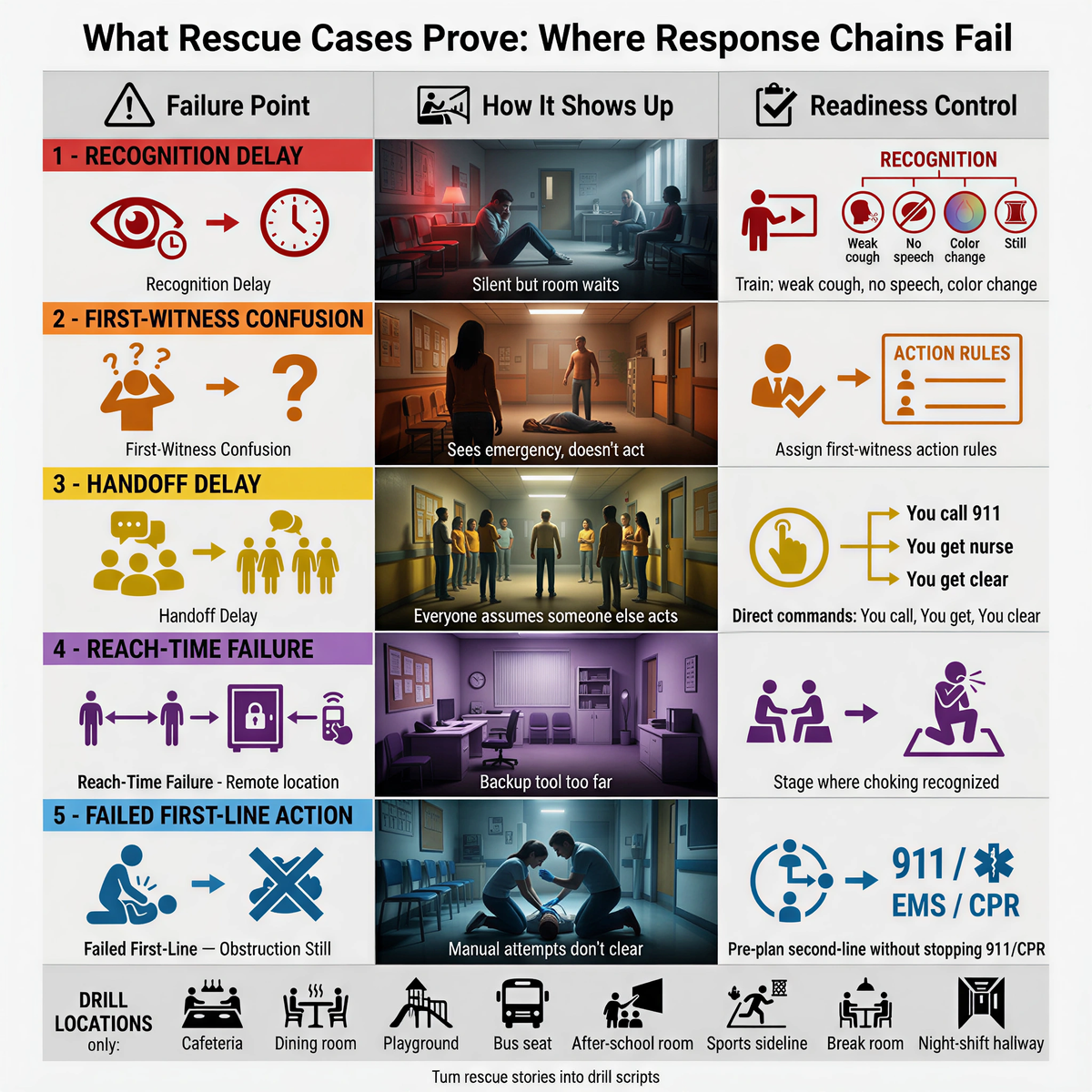
They show where response chains fail.
|
Failure point |
How it shows up |
Readiness control |
|
Recognition delay |
The child, resident, or guest goes silent, but the room waits for a louder sign |
Train staff to recognize weak cough, no speech, color change, sudden stillness, and distress |
|
First-witness confusion |
The closest person sees the emergency but does not know whether to start care or call someone |
Assign first-witness action rules by role and room |
|
Handoff delay |
Everyone assumes someone else called 911 or retrieved help |
Use direct commands: "You call 911," "You get the nurse," "You clear the aisle" |
|
Reach-time failure |
The backup tool is in an office, cabinet, or remote station |
Stage second-line resources where choking is most likely to be recognized |
|
Failed first-line action |
Manual attempts start but do not clear the obstruction |
Pre-plan the second-line decision point without stopping 911, EMS, or CPR readiness |
The wrong lesson from a successful rescue is “someone like that will probably be nearby.”
The better institutional habit is to turn the story into a drill script.
Run the scene with the first witness as a cafeteria monitor, dining aide, babysitter, server, substitute teacher, hotel breakfast attendant, banquet worker, bus aide, night-shift caregiver, or family member. Measure how long it takes to recognize severe choking, start first-line care, call 911, and reach any staged second-line backup.
Repeat the drill from the far table, the back booth, the playground snack bench, the memory-care dining corner, the staff break room, the classroom snack area, and the night-shift hallway.
If the first responder has to leave the person, find a key, cross a crowded room, or guess where the airway emergency kit is stored, the response chain is already losing time.
A rescue case is not reassurance. It is a prompt to test the room.
The buying question should not start with “Does the device exist?”
A serious buyer asks a harder set of questions.
A second-line airway device has value only inside a working response chain. Without training, role clarity, placement logic, and documentation, the product becomes another item in a cabinet.
For related planning context, review the anti-choking device buyer evidence checklist.
For related planning context, review the classroom snack table.
No. Rescue cases should be read inside the established sequence. Manual first-line choking rescue, 911 activation, and CPR readiness still come first. A QXN suction anti-choking device is a second-line backup after unsuccessful BLS choking protocol.
They show where the response chain bends in real rooms: recognition delay, first-witness uncertainty, handoff delay, reach-time to backup, and confusion after failed first-line action.
It is the backup step after established manual choking first aid has been attempted without success in a complete airway obstruction emergency. It may include a policy-authorized QXN suction anti-choking device if available, trained, and reachable.
Audit recognition speed, first-line competence, 911 delegation, device reach-time, handoff clarity, CPR readiness, and whether the plan still works during lunch, after-school coverage, dining service, overnight staffing, or high-crowd events.
It shifts the buying question from “Does the device exist?” to “Can the right person reach and use it after first-line care fails, without delaying 911, CPR, or standard rescue steps?”
Yes, but only if it becomes a drill. The team should map the room, assign first-witness roles, measure retrieval time, practice 911 delegation, and identify the point where second-line anti-choking device backup may enter after failed first-line care.
It should be staged based on reach-time from likely choking locations, not administrative convenience. Cafeterias, dining rooms, snack areas, restaurant floors, memory-care units, hotel breakfast zones, and staff break rooms may require different placement logic.
FDA Safety Communication, March 4, 2026
American Heart Association 2025 CPR/ECC updates
WTOP Lusby infant rescue report
KMBC assisted-living dining-room rescue report
This article is for education and institutional readiness planning only. It is not medical, legal, regulatory, or procurement advice. In a choking emergency, call 911, follow dispatcher instructions, use current first-aid training, and follow device labeling and facility policy.




















