OSHA compliance in medical deserts turns on time, not geography. When outside aid can't reach a remote route or worksite inside OSHA's 3 to 4 minute window for life-threatening events, the employer needs an on-site rescue chain: trained first responders, ready first-aid supplies, and, where first-line airway response can fail, a second-line backup layer.
29 CFR 1910.151(b) is short. If an infirmary, clinic, or hospital is not in 'near proximity' to the workplace and used for treatment of injured employees, the employer must have one or more adequately trained first-aid responders and adequate first-aid supplies readily available.
OSHA never intended that sentence to be satisfied by a mailing address. The agency's interpretation letters keep returning to the same practical test: how long does it take for meaningful aid to reach the injured worker where the event actually happens?
Remote yards, rural routes, mobile crews, school transport fleets, and satellite depots expose the weak reading immediately. A clinic can exist in the county and still be useless inside the biological window that matters for stopped breathing or complete airway obstruction.
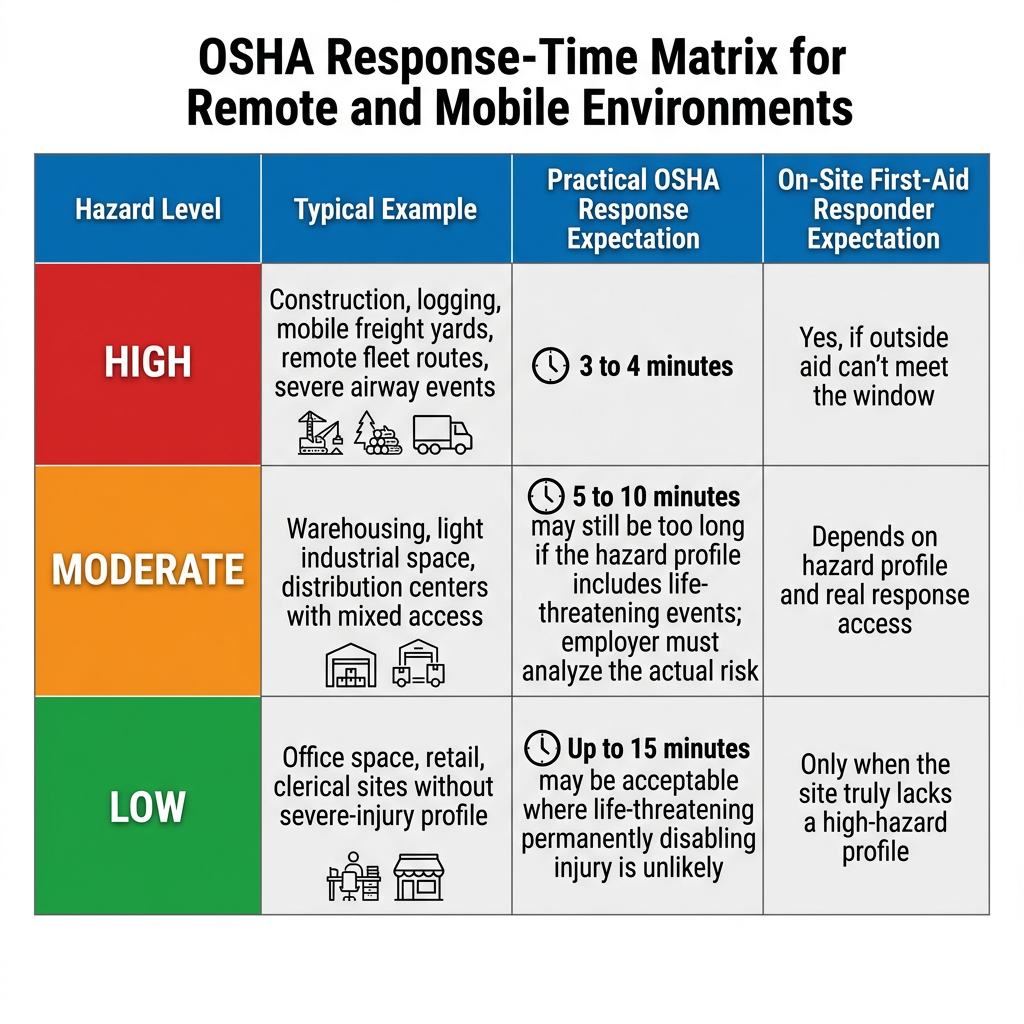
OSHA's interpretation letters have been remarkably consistent. For suffocation, stopped breathing, severe bleeding, and other life-threatening conditions, first aid has to be available within 3 to 4 minutes from the time of injury to the time aid is administered. OSHA has also said a longer interval, such as 15 minutes, may be acceptable where life-threatening or permanently disabling injury is unlikely.
Distance redefines liability in mobile fleets and remote worksites. A nearby clinic on a map doesn't help if dispatch, turnout, gate access, unpaved roads, weather, or route position push actual care well past the oxygen window.
|
Hazard level |
Typical example |
Practical OSHA response expectation |
On-site first-aid responder expectation |
|
High |
Construction, logging, mobile freight yards, remote fleet routes, severe airway events |
3 to 4 minutes |
Yes, if outside aid can't meet the window |
|
Moderate |
Warehousing, light industrial space, distribution centers with mixed access |
5 to 10 minutes may still be too long if the hazard profile includes life-threatening events; employer must analyze the actual risk |
Depends on hazard profile and real response access |
|
Low |
Office space, retail, clerical sites without severe-injury profile |
Up to 15 minutes may be acceptable where life-threatening or permanently disabling injury is unlikely |
Only when the site truly lacks a high-hazard profile |
OSHA does not publish one fixed matrix for every industry. The table above translates the agency's interpretation letters into an operational screen for remote and mobile settings. Life-threatening hazards sit in the 3 to 4 minute lane.
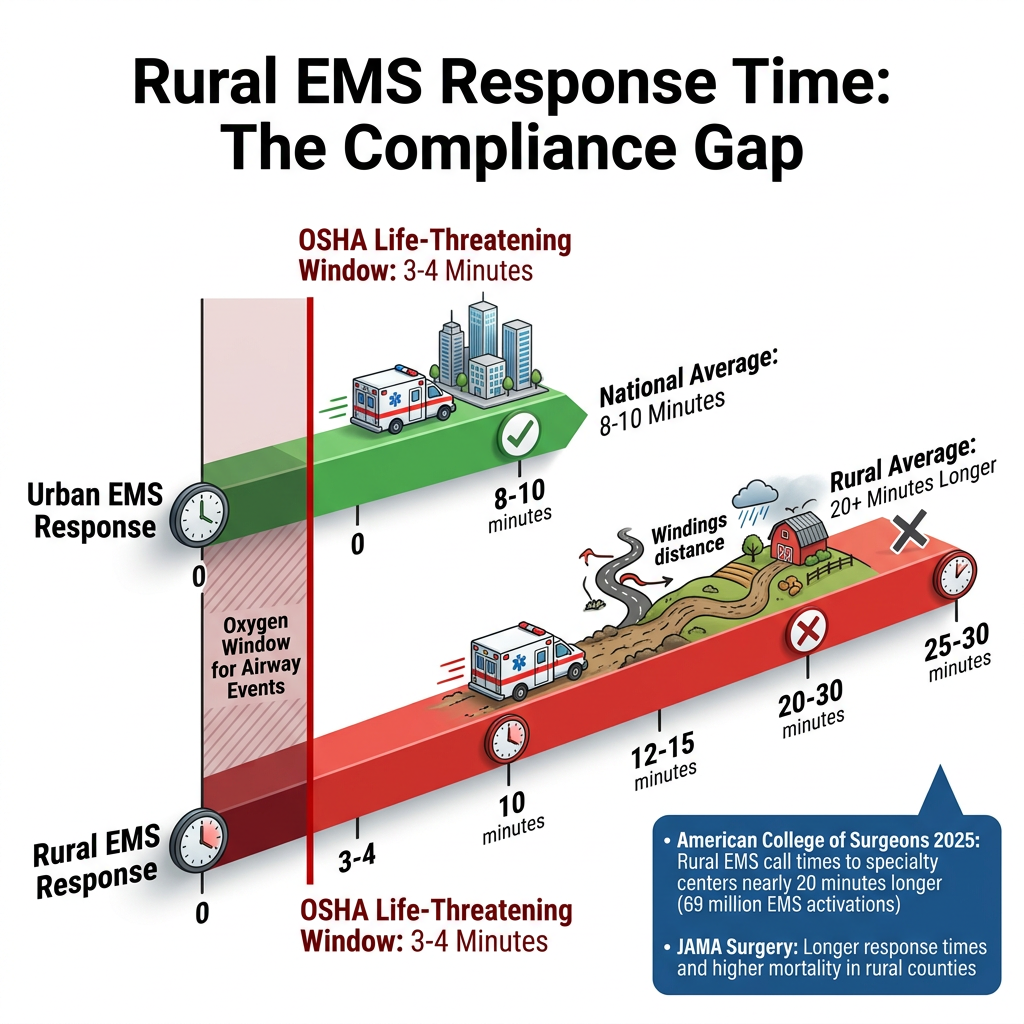
The American College of Surgeons reported in 2025 that rural EMS call times to specialty centers were nearly 20 minutes longer than the national average in a study built on almost 69 million EMS activations. Earlier national work in JAMA Surgery also found longer response times and higher mortality in rural and wilderness counties.
Those datasets are not airway-only. They do not need to be. They answer the compliance question that remote operators keep trying to avoid: outside medical aid often arrives after the time window OSHA uses for life-threatening emergencies. Once that is true, the employer's first-aid program has to carry more weight on site.
A medical desert is not defined by whether a town has a clinic. It is defined by whether meaningful aid can reach the worker before hypoxia, exsanguination, or irreversible injury outruns the response.
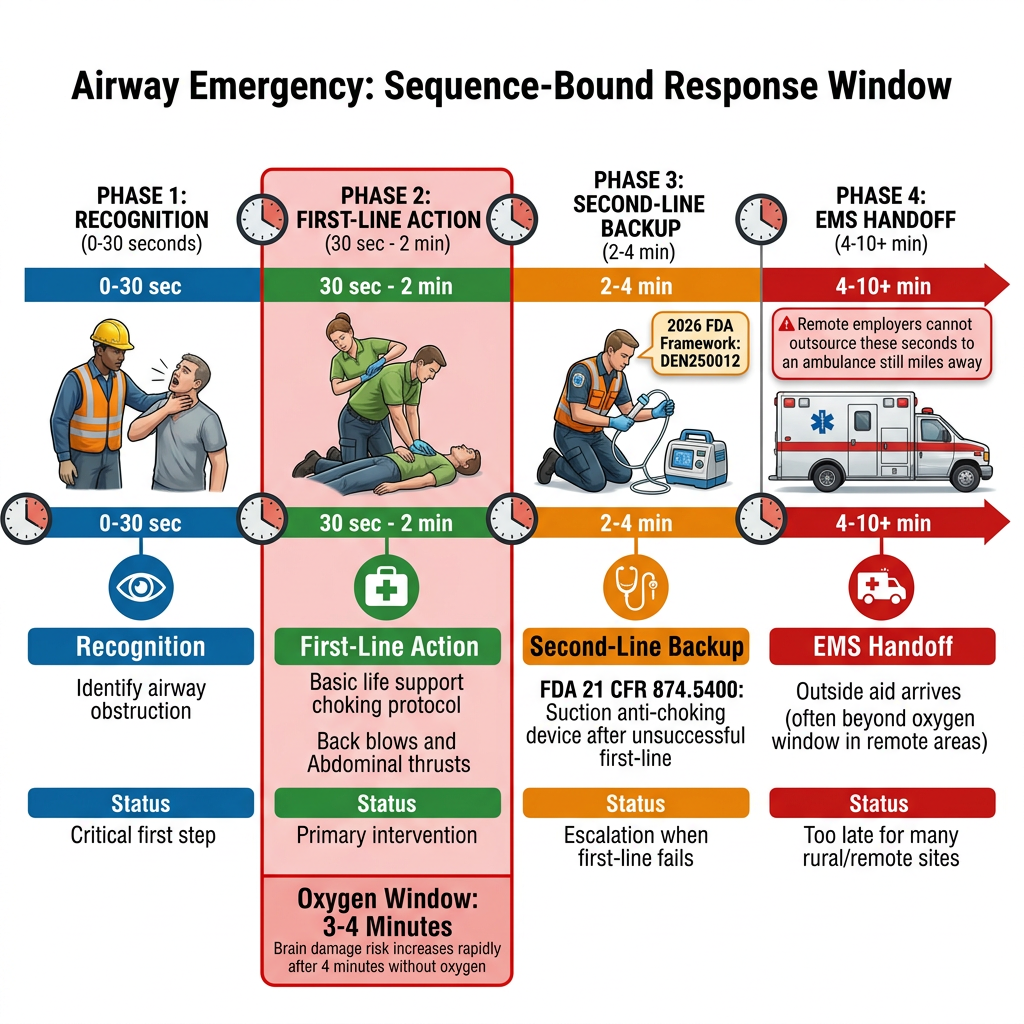
OSHA's letters speak in general terms such as stopped breathing and suffocation. A severe airway obstruction belongs in that class. The first seconds are sequence-bound: recognition, first-line action, escalation if the obstruction does not clear. A remote employer cannot outsource those seconds to an ambulance that is still several miles away.
The 2026 FDA framework matters here because it finally defined a lawful second-line device category. Under DEN250012, FDA created 21 CFR 874.5400 for a 'suction anti-choking device as a second-line treatment' after unsuccessful use of a basic life support choking protocol. That classification did not change OSHA's first-aid rule. It did give employers and safety teams a cleaner way to define a backup layer when first-line action does not resolve the event.
First-line response still owns the opening window. Training has to reflect that. A remote operation that places all of its confidence in 911 or in an unopened device kit is still reading the standard too loosely.
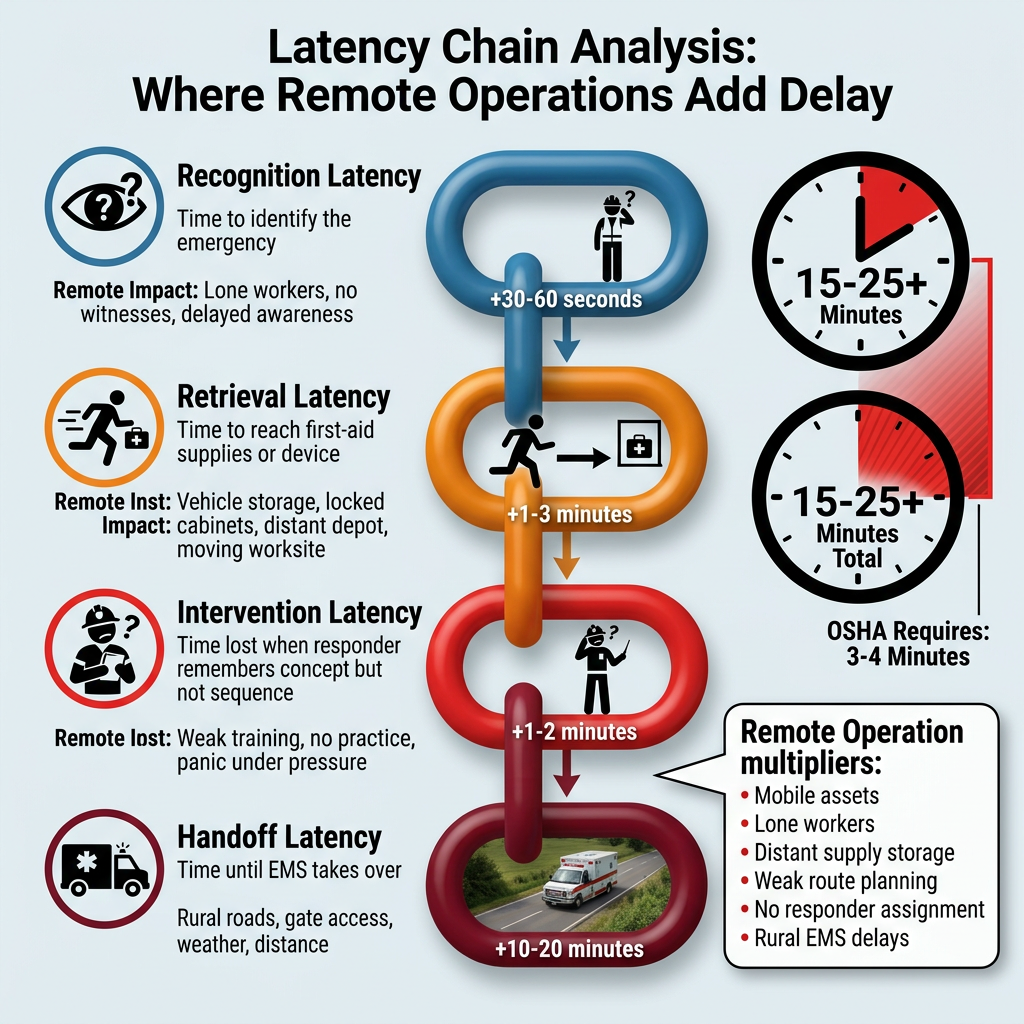
Fitiger's engineering and product safety team reads remote airway readiness through Latency Chain Analysis. The delay is never one number. Recognition latency sits first. Retrieval latency follows. Intervention latency appears when the responder remembers the concept but not the sequence. Handoff latency arrives when EMS finally takes over. Each link adds time. Remote operations stretch all four.
A general first-aid certificate at headquarters does not shorten the chain for a driver on a rural shoulder. A stocked cabinet in the depot does not shorten the chain for a lone yard worker at an outlying transfer point. Weak route planning, weak responder assignment, and weak equipment staging all widen the gap before an intervention even starts.
Reading medical deserts requires this lens: the issue isn't the presence of a clinic, but the accessibility of aid within the 4-minute oxygen window. Mobile assets break weak plans faster because the worksite itself keeps moving.
A real plan answers plain questions. Who on this shift is trained? Where is the kit stored on the vehicle or at the site? Who starts first-line action? What happens if the only trained person is the one directly involved in the event? How long does it take to reach supplies from the likely incident point?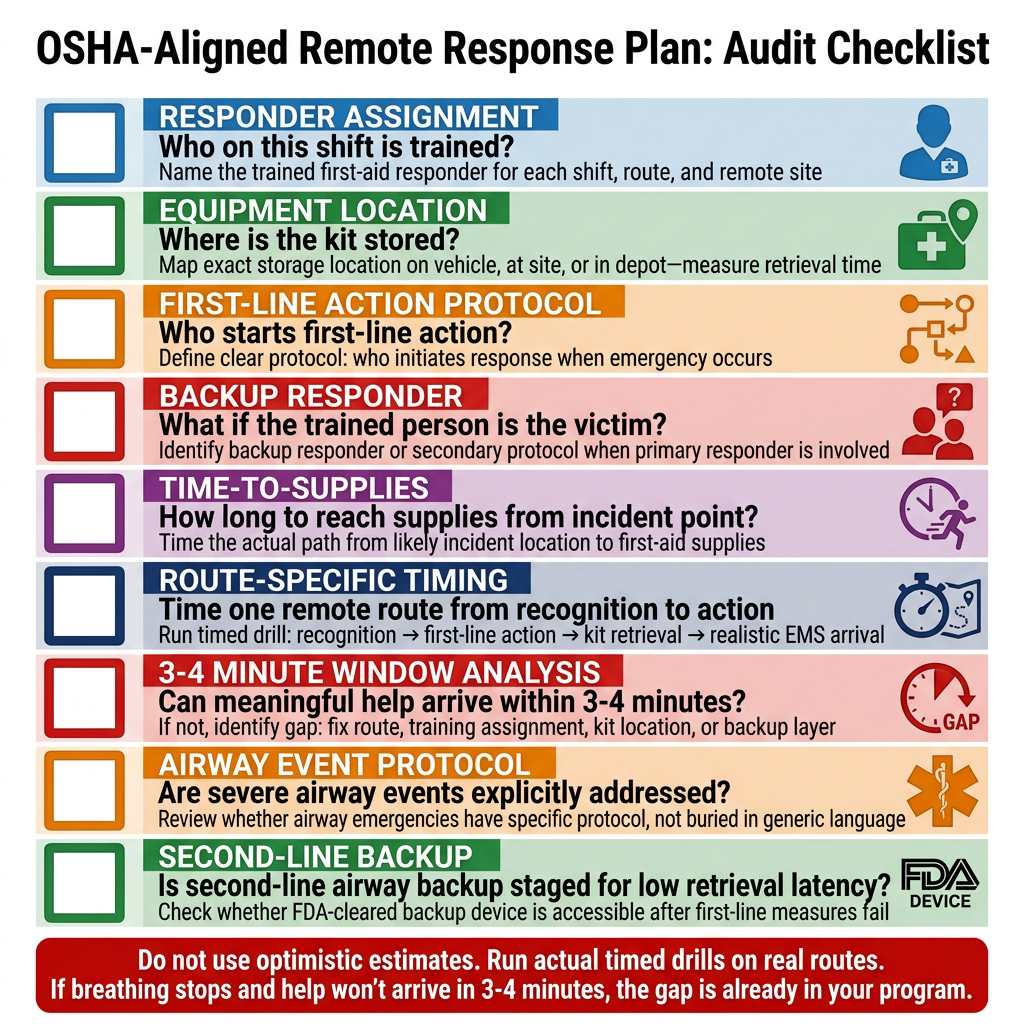
Remote fleet programs need route-specific answers, not headquarters assumptions. School bus systems, long-haul routes, field service vehicles, and rural depots all need their own deployment logic. A first-aid cabinet in the base building does not protect the worker or passenger who is already away from it.
OSHA's first-aid training interpretations also push toward role clarity. Workers should understand the employer's actual plan for medical emergencies, not simply hold a generic certificate with no operational assignment.
Pick one remote route this week. Run a timed drill. Record recognition time, time to first-line action, time to the kit, and nearest realistic EMS arrival. Do not use the optimistic estimate.
If the worker would not have meaningful help inside 3 to 4 minutes when breathing stops, the gap is already inside your program. Fix the route, the training assignment, the kit location, or the backup layer before you buy anything else.
Download the Remote & Mobile Readiness Toolkit
When help may be minutes away, readiness has to be planned before the emergency.
Download the Remote & Mobile Airway Safety Readiness Toolkit to map delays, assign roles, plan equipment access, and prepare your team for choking emergencies in rural, mobile, or field-based environments.
Does OSHA require a hospital to be within 3 to 4 minutes of every remote worksite?
No. OSHA requires adequately trained first-aid responders and readily available first-aid supplies when an infirmary, clinic, or hospital is not in near proximity. The agency's interpretation letters use 3 to 4 minutes for life-threatening events as the practical benchmark for near proximity.
Do rural EMS delays automatically create an OSHA violation?
Not by themselves. The problem appears when the employer relies on outside aid that cannot reach the worker inside the biologically useful window for a life-threatening emergency and has not built an on-site first-aid response to close that gap.
Does OSHA 29 CFR 1910.151 specifically require a second-line airway device?
No. The standard speaks in terms of trained responders and first-aid supplies. A second-line airway device becomes relevant only as a backup layer after first-line response, especially where remote conditions make outside aid too slow.
Why does route-specific planning matter more than headquarters distance?
Because near proximity is judged by the worker's actual access to aid, not by how close the main office sits to a clinic. Dispatch delay, road access, vehicle location, and shift patterns all change the real response window.
What should a remote employer measure first?
Start with the real timeline: recognition to first-line action, worker to supplies, and realistic EMS arrival from the point where the event is most likely to happen.
This article is for educational and operational planning purposes only. It does not provide medical, legal, or regulatory advice. Employers should follow current OSHA requirements, site-specific hazard assessments, state and local law, and current first-aid and emergency-response guidance. In any real emergency, call 911 and begin trained first-line response immediately.




















