Pregnancy doesn't automatically make every meal dangerous. Some situations can become less forgiving, especially when reflux, nausea, fatigue, uncomfortable posture, or large prenatal vitamins are already making swallowing harder.
If a pregnant person can't speak, cough effectively, or breathe normally, call 911 and begin choking first aid immediately.
A late dinner on the couch can feel like the most ordinary moment of the day.
The kitchen is finally quiet. Shoes are off. A plate rests on the coffee table. A pregnant person takes a quick bite while leaning back into the cushions, tired enough to eat faster than usual.
For a household checklist, see Fitiger's child and home choking safety readiness plan.
Then the swallow doesn't go the way it should.
A cough starts, but it doesn't sound strong. The room changes. A partner looks over and realizes that the person on the couch is trying to speak but can't.
Most pregnancy choking emergencies do not begin with an obviously reckless decision. They begin inside routines that feel harmless: a dry bite after a long day, a large pill swallowed too quickly, or a meal eaten alone while distracted.
Pregnancy is not a diagnosis of swallowing difficulty.
Many pregnant people eat normally throughout pregnancy and never experience a choking emergency. The practical concern is narrower: pregnancy can change comfort, posture, appetite, and daily routines. Reflux may make certain meals unpleasant. Nausea may lead to rushed eating. Fatigue may make the couch more appealing than the dining table. Large prenatal vitamins may become harder to swallow than expected.
None of those conditions guarantees a choking event.
They do create moments where a slower pace and a more deliberate setup make sense.
If swallowing food, liquids, or pills is becoming difficult repeatedly, bring it up with a clinician. Persistent trouble swallowing deserves medical attention rather than a series of improvised workarounds at home.
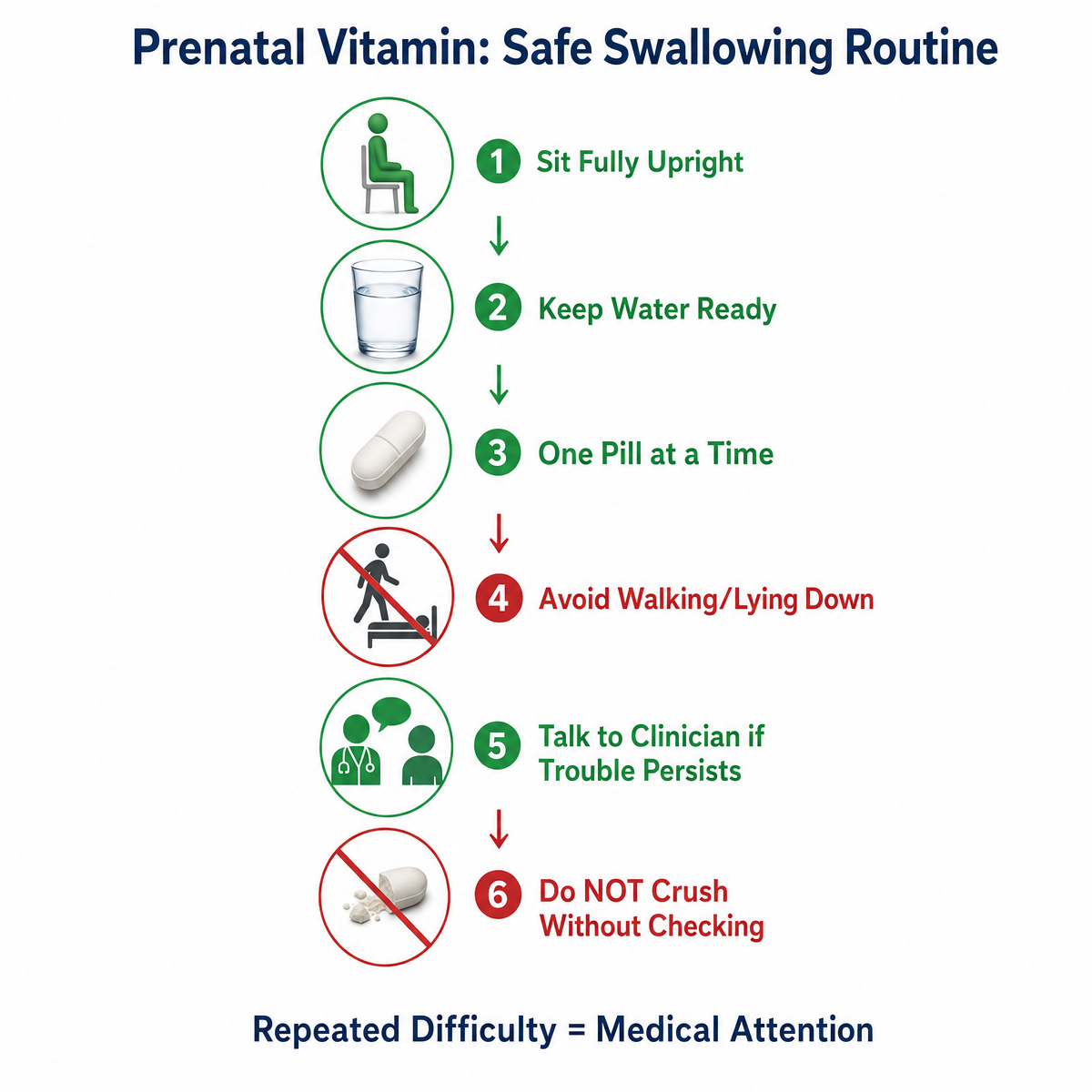
A prenatal vitamin may be part of an everyday routine, but it can still be difficult to swallow.
The problem often appears when the pill is taken quickly, without enough water, or while someone is already nauseated or exhausted. A large tablet that went down easily earlier in pregnancy may become more uncomfortable later.
A steadier routine helps:
Some prenatal supplements are available in different forms, but the right alternative depends on the person and the product. Repeated difficulty is not something to push through indefinitely.

A couch is comfortable. It is not always the best place for a hurried meal.
Late in pregnancy, many people shift positions constantly to stay comfortable. Meals may happen half-reclined because sitting at the table feels like one task too many. A dry sandwich, dense piece of meat, or large bite of bread can be harder to manage when the body is tilted back and the person is tired.
The practical rule is simple:
|
Sit upright while eating and slow down the first few bites. |
That does not require a rigid posture or a clinical feeding setup. It means giving swallowing a fair chance instead of adding avoidable strain to an already uncomfortable meal.
Water can help with ordinary dryness during a meal. It is not a treatment for a blocked airway. If severe choking begins, do not offer a drink. Start emergency action.
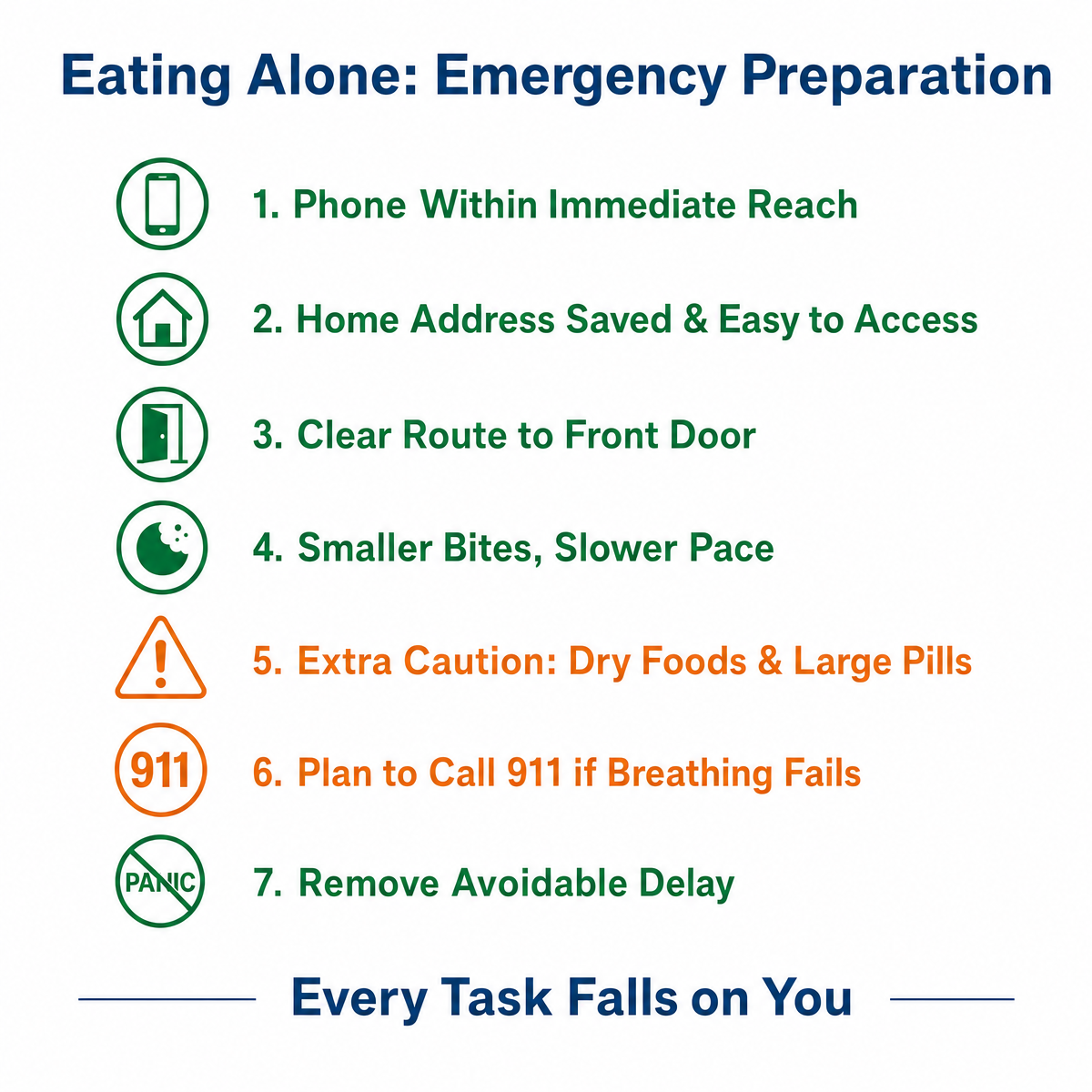
Eating alone is not inherently unsafe. The problem is what happens if a meal suddenly turns into an emergency.
When another adult is nearby, one person can call 911 while the other starts first aid. Someone can unlock the door, turn on an outside light, or direct responders to the right room.
When the pregnant person is alone, every task falls on the person who is already struggling to breathe.
A realistic solo-meal setup includes:
The point is not to make solo meals feel frightening. It is to remove avoidable delay.
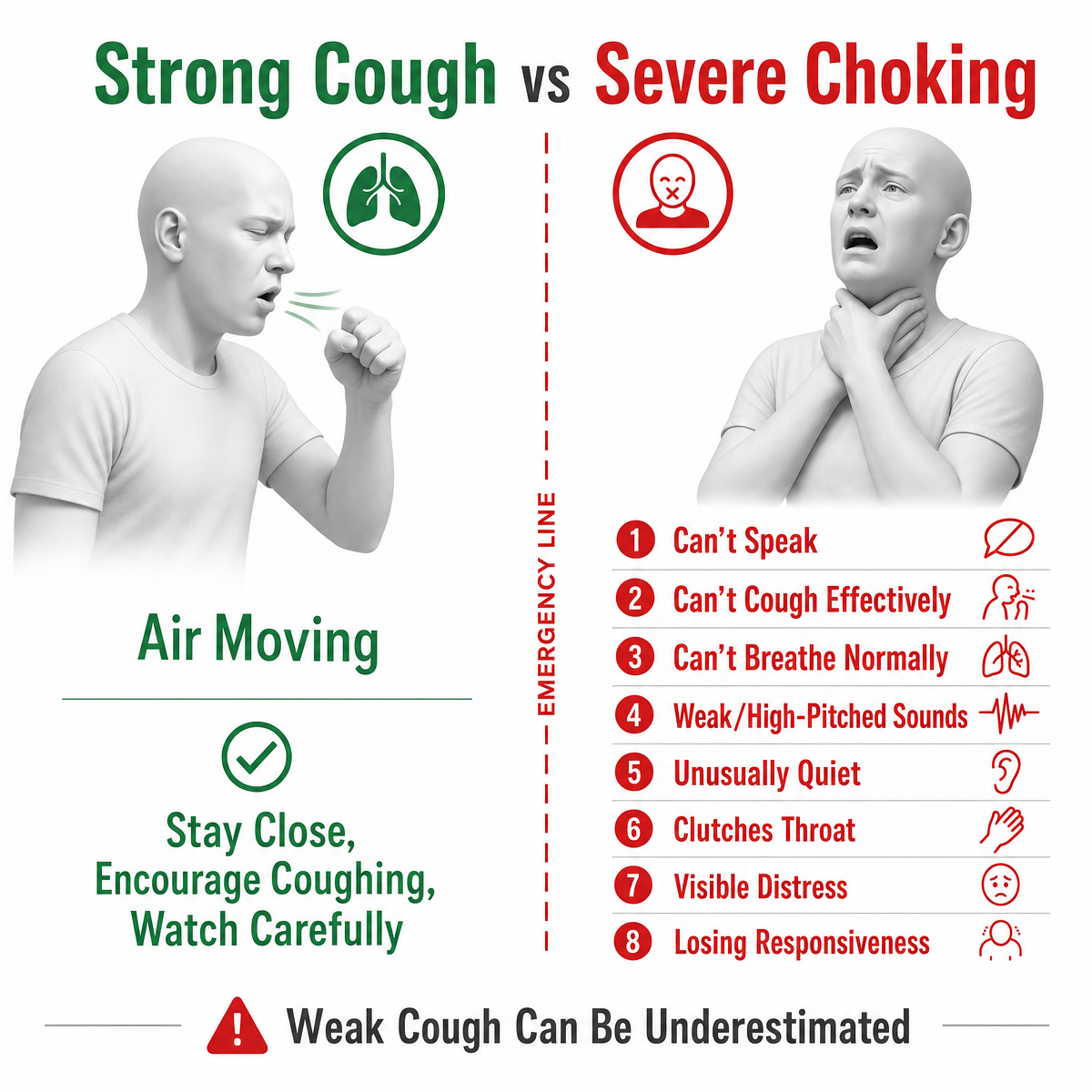
A person who is coughing forcefully is still moving air.
Stay close. Encourage continued coughing. Watch carefully for a change. Do not offer food or water. Do not reach blindly into the mouth.
Severe choking looks different. Treat the situation as an emergency if the person:
A weak cough can be easy to underestimate because it still sounds like an attempt to clear the airway. The important question is whether air is actually moving effectively.
For a responsive adult with severe choking:
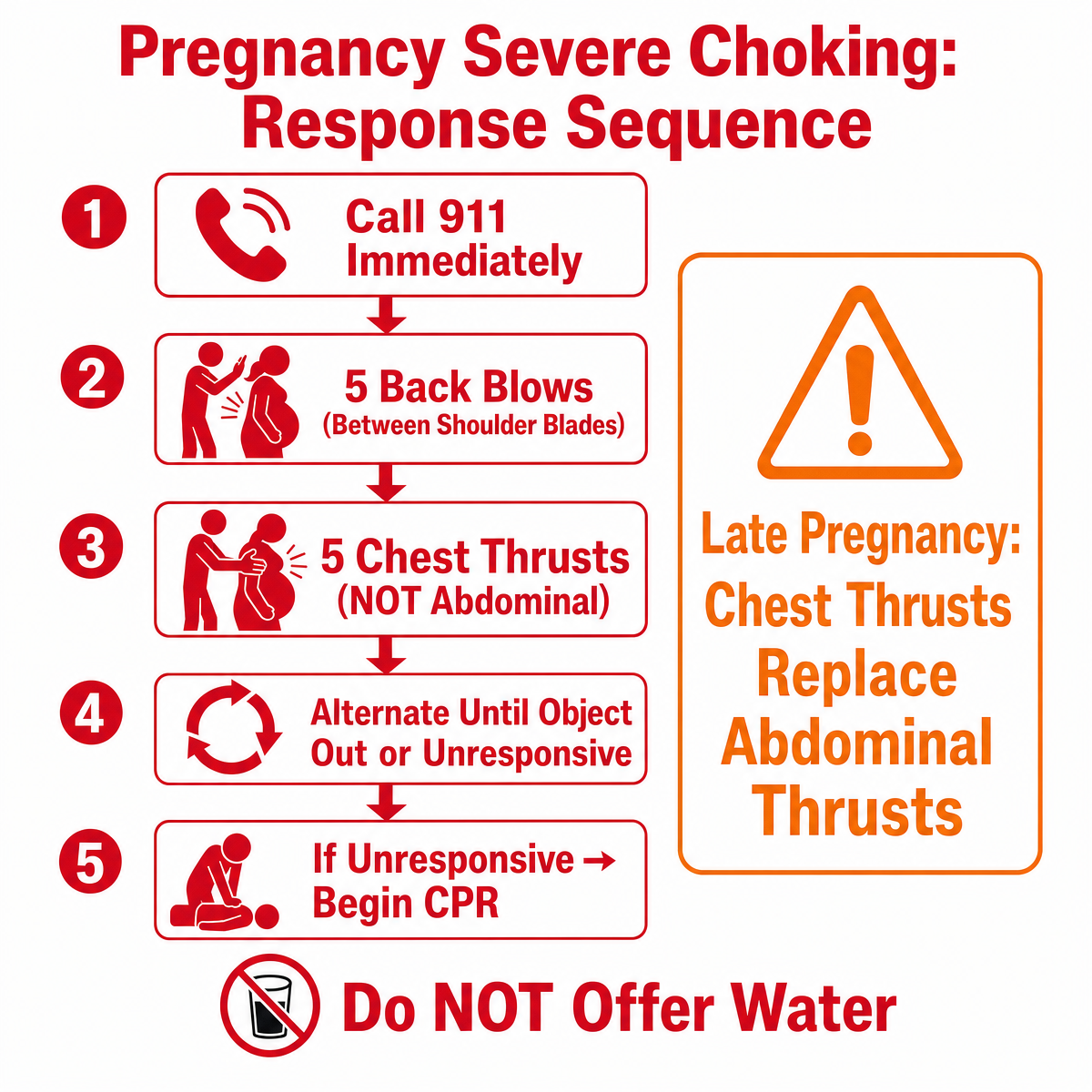
American Red Cross materials also instruct responders to use chest thrusts instead of abdominal thrusts when a person is obviously pregnant or known to be pregnant.
Only remove an object from the mouth if you can clearly see it. Do not perform a blind finger sweep.
The distinction matters because a pregnant person's body changes how the response is performed. Guessing under pressure is a poor substitute for hands-on training.
Offering water feels natural when someone appears to have food stuck in the throat.
For severe choking, it wastes time.
A person who cannot speak, cough effectively, or breathe normally needs emergency first aid, not another swallow. Do not hand over a drink. Do not offer more food. Do not wait to see whether the blockage clears on its own.
Call 911 and begin the appropriate choking sequence.
A suction anti-choking device does not replace 911, manual choking rescue, CPR, or first-aid training.
Current FDA guidance allows anti-choking devices to be considered as a second option after established choking rescue protocols have been attempted without success. Current AHA guidance also makes an important point: the effectiveness and safety of suction-based airway-clearance devices in adults with severe foreign-body airway obstruction have not been established well enough for a recommendation.
A household that keeps one should treat it as a backup only.
The order should remain clear:
|
Call 911. Begin trained choking first aid. Consider a suction device only as a second-line backup after standard rescue is unsuccessful. Begin CPR if the person becomes unresponsive. |
Do not delay trained first aid while searching for a device.
Many households have never discussed how choking first aid changes during pregnancy.
A partner may remember abdominal thrusts from an older class or a television scene. A parent visiting for the weekend may not know that chest thrusts are used instead in late pregnancy. A roommate may not know where the home address is written down.
A short conversation removes several weak points:
A plan that exists only in one person's head is fragile.
A safer routine does not require turning every meal into a safety exercise.
Start with the moments that are already uncomfortable:
Small adjustments are easier to keep using because they fit inside normal life.
Look at the place where late-night meals usually happen.
If the couch is the default, sit more upright. If prenatal vitamins keep catching in the throat, stop treating it as a minor annoyance and ask about alternatives. If meals often happen alone, place the phone where it can be reached without crossing the room.
Then make sure the people nearby know the emergency sequence.
When speech, effective coughing, or normal breathing disappears, the next step should not need to be invented in the moment.
No. Pregnancy does not make every meal dangerous. The practical concern is that reflux, nausea, fatigue, posture discomfort, or difficulty swallowing large pills may create situations that deserve more care.
Call 911 immediately and begin choking first aid. Give 5 back blows. In late pregnancy, or when the abdomen cannot be encircled safely, follow with 5 chest thrusts instead of abdominal thrusts. Continue until the object clears or the person becomes unresponsive.
For late pregnancy, current AHA guidance uses chest thrusts instead of abdominal thrusts. American Red Cross materials also direct responders to use chest thrusts when a person is obviously pregnant or known to be pregnant.
Large pills can be difficult for some people to swallow. Sit upright, use enough water, take pills one at a time, and speak with a clinician or pharmacist if the same prenatal vitamin repeatedly causes difficulty.
Not if the person cannot speak, cough effectively, or breathe normally. Water will not clear a blocked airway and may delay emergency action.
A strong cough usually means air is still moving. Encourage coughing and stay close. If the cough becomes weak, ineffective, or silent, or normal breathing and speech disappear, treat it as severe choking.
No. Call 911 and begin trained choking first aid first. FDA guidance places anti-choking devices in a second-option role after established protocols have failed. AHA guidance says the evidence is still insufficient to recommend suction-based airway-clearance devices for adults with severe choking.
When should difficulty swallowing be discussed with a clinician?
Talk with a clinician if food, liquids, or pills repeatedly feel difficult to swallow, if coughing happens often during meals, or if swallowing discomfort is becoming more frequent rather than resolving.
Resources
American Heart Association - Part 7: Adult Basic Life Support
American Heart Association - Adult Foreign-Body Airway Obstruction Algorithm
American Red Cross - Adult and Child Choking: Symptoms and First Aid
FDA - FDA Encourages the Public to Follow Established Choking Rescue Protocols
Medical and Safety Disclaimer
This content is for general education and emergency-preparedness planning only. It does not replace medical advice, diagnosis, treatment, legal advice, certified first-aid or CPR training, dispatcher instructions, EMS or 911, professional care, or any product-specific instructions for use. Call 911 immediately for severe choking. Follow current certified training and dispatcher guidance. FITIGER products must not be treated as replacements for prevention, manual choking rescue, CPR, or emergency medical care. Any suction anti-choking device belongs in a second-line backup role only after established rescue protocols have been attempted without success and only within the product-specific instructions for use.




















