What matters mostA purchase order doesn't make a campus safer by itself. The real shift in 2026 came from the FDA. Suction anti-choking devices now sit inside a defined federal category as a second-line treatment. That changed the conversation for schools. Procurement now has to live next to BLS training, placement decisions, documentation, and audit-ready records. That also changed what 'compliant' looks like. Schools can't treat these devices as generic emergency products anymore. Device status, training expectations, grant language, sole-source justification, accounting treatment, and post-use reporting all matter now. The work moved out of a single budget line and into a full safety workflow. Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions. |
The easiest mistake is still the one districts make first. A device gets purchased, mounted, and quietly assumed to have solved the problem.
It hasn't.
A second-line device enters the picture only after standard choking response fails. That's not a marketing line. That's the federal frame. Once that line hardened in 2026, school procurement changed with it. The device stopped being a standalone safety purchase and became part of a sequence: recognition, BLS, retrieval, use, documentation, review.
That's the sequence campuses have to build now. Not a wall display. Not a box checked in a meeting. A sequence.
Most district leaders don't need a seminar on device law. They need the practical version.
The FDA didn't create a replacement for first-line choking response. It defined a second-line tool. That one distinction reshaped school purchasing. A district can no longer talk about airway devices as if they sit outside training, storage, documentation, or post-incident review. Once the tool is second-line by definition, everything around it has to prove the campus can reach it late enough to respect BLS and early enough to matter.
That's where 2026 stopped being a product conversation and turned into a systems conversation.
A school can buy a wall station in an afternoon. Building a reliable response around it takes longer.
Packaging matters. Assembly time matters. Staff confidence matters. The route from cafeteria table to wall cabinet matters. The nurse's office being one hallway too far matters. A lunch monitor freezing for five seconds because nobody has shown them exactly when BLS stops and device use begins matters.
Teams still drift toward hardware first because hardware is visible. Training logs, role clarity, and retrieval timing aren't. Real emergencies expose that mistake fast. A second-line framework only works when first-line response is clear, fast, and practiced. BLS first. Device second. No confusion in the middle.
Schools usually separate these conversations. One room talks about safety. Another talks about grants. Another handles purchasing. Finance gets pulled in later. That split gets expensive.
In 2026, districts looking at airway readiness usually end up dealing with two very different funding stories. COPS SVPP fits hardware, site upgrades, and physical safety measures. BJA STOP fits training, protocol development, reporting systems, and prevention programming. Trying to force both needs through one narrative weakens the file and muddies the purpose of the request.
The practical question isn't just 'Can we pay for this?' It's 'Which part of the system are we funding?' The answer changes the grant path, the internal memo, the coding choice, and the records the district will need later.
A lot of teams hear 'only one authorized product' and jump straight to sole-source. That's not enough.
Single-source purchasing still has to survive scrutiny. The procurement file has to show why the product's regulatory status matters, why that status affects the district's compliance position, and why a broader bid field doesn't solve the problem right now. The work doesn't end at 'there's only one.' It starts there.
Before March 2026, internal review often drifted into product claims and brand comparisons. After March 2026, the memo got sharper. Authorized status. Intended use. Training implications. Procurement defensibility.
Federal classification created a floor. States are already shaping what schools may have to do with it.
Texas SB 57 pushed school safety planning harder toward disability accommodation. That matters for airway safety because swallowing risk, mobility limits, and dining-room logistics don't land evenly across all students. A device placed for the average hallway may fail the student most likely to need a better plan.
Placement can't stay generic. Some campuses need a tighter map. Some students need a tighter response plan. Some drills need a completely different design.
The dramatic part is obvious. Emergency. Airway obstruction. Seconds matter.
The boring part decides whether those seconds get wasted.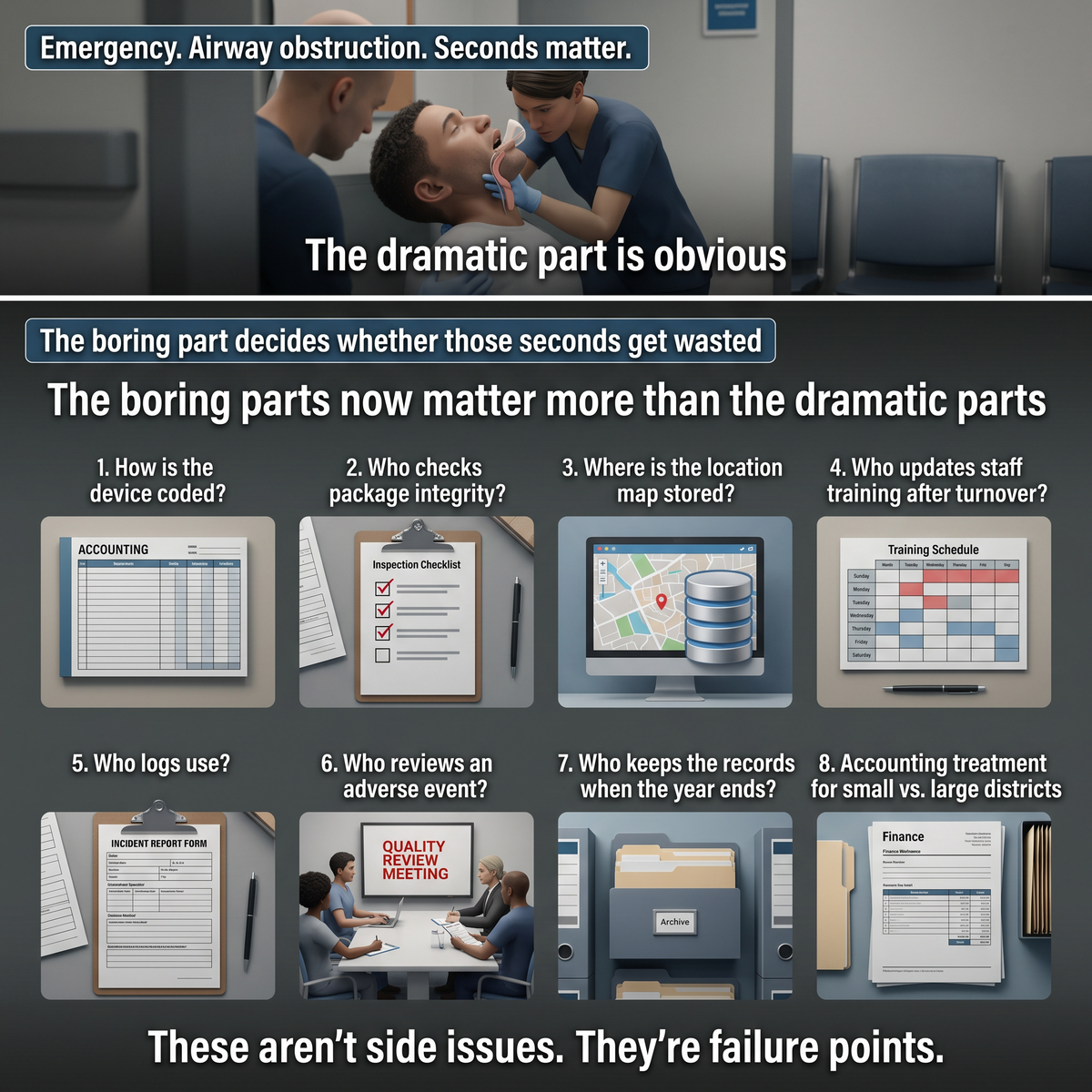
How is the device coded? Who checks package integrity? Where is the location map stored? Who updates staff training after turnover? Who logs use? Who reviews an adverse event? Who keeps the records when the year ends and the people who handled the rollout have moved on?
These aren't side issues. They're failure points. The same goes for accounting treatment. Small districts may record these purchases one way. Large districtwide buys may trigger different tracking rules, inventory controls, or capitalization questions. Finance can't be the last stop anymore. It has to be in the room before the order goes out.
Start with risk, not catalog pages.
Look at meal settings. Look at nurse office distance. Look at special education needs. Look at lunch staff coverage. Look at the periods when complete obstructions are most likely to happen. Look at whether current BLS training is real, current, and role-specific. Look at whether the district already has a clean path for documenting equipment, training, and post-use review.
Then buy.
The strongest purchases in 2026 won't come from fear or trend pressure. They'll come from districts that can explain the whole chain: why this campus needs a school choking emergency kit, why the chosen product meets the right standard, how staff are trained, where the unit sits, how it gets documented, and what happens after use.
Picture the scene nobody wants but every district should be planning for anyway.
Lunch period. Noise. A complete obstruction. BLS starts. Someone moves for the device without asking where it is because the location was fixed months ago. Nobody is opening a cabinet for the first time. Nobody is reading the package for the first time. Nobody is arguing about whether they're allowed to act.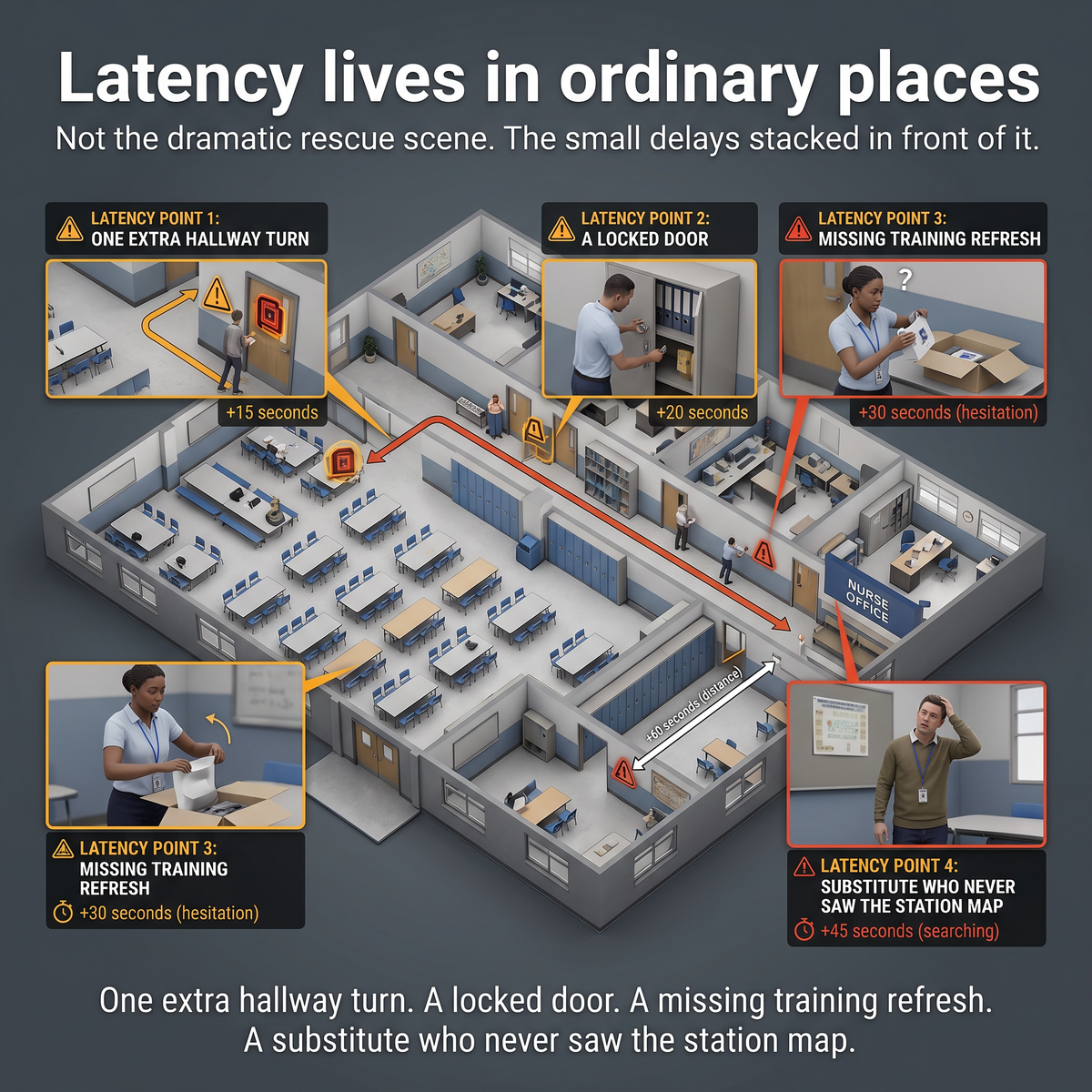
Latency lives in ordinary places. One extra hallway turn. A locked door. A missing training refresh. A substitute who never saw the station map. A campus plan that looked complete until a real student couldn't fit the assumptions built into it.
Those are the failure points. Not the dramatic rescue scene. The small delays stacked in front of it.
That's the real point of the 2026 shift. Not a new gadget. A tighter system that leaves less room for hesitation, misplacement, and wasted seconds when the first line fails and the second line has to be there.
What changed for schools after 21 CFR 874.5400?
Schools now have a clearer federal reference point for evaluating suction anti-choking devices. The practical change is that these devices are defined as second-line tools, not replacements for first-line choking response.
Can a school buy a device without changing its training plan?
It can, but that's weak practice. A second-line framework only works if staff already understand first-line BLS response, retrieval timing, and device-use sequence.
Which federal funding path is usually more relevant for hardware?
COPS SVPP is generally the closer fit for physical safety measures and equipment-related planning, while BJA STOP is usually better aligned with training, reporting systems, and prevention programming.
Does 'only one authorized product' automatically make sole-source purchasing valid?
No. A district still needs a documented procurement rationale that explains why the product's regulatory status matters and why the purchase approach is defensible under its procurement rules.
Why do accounting and audit issues matter for a safety device?
Because the device has to be coded, tracked, documented, and reviewed inside the same purchasing, inventory, and record-retention systems that govern other safety spending.
2) FDA De Novo Order (DEN250012)
4) COPS School Violence Prevention Program
5) FY25 SVPP Opportunity Listing
6) BJA STOP School Violence Program
7) Texas SB 57 Coverage for 2025-2026 School Year
8) Texas SB 57 Bill Text / Status Reference
This article is for educational and operational planning purposes only. It does not provide medical or legal advice. Schools should follow current American Heart Association or Red Cross choking-response guidance, district policy, applicable procurement rules, and the latest federal and state requirements. In any real emergency, call 911 and activate trained first-line response immediately.




















