Key Takeaway |
|
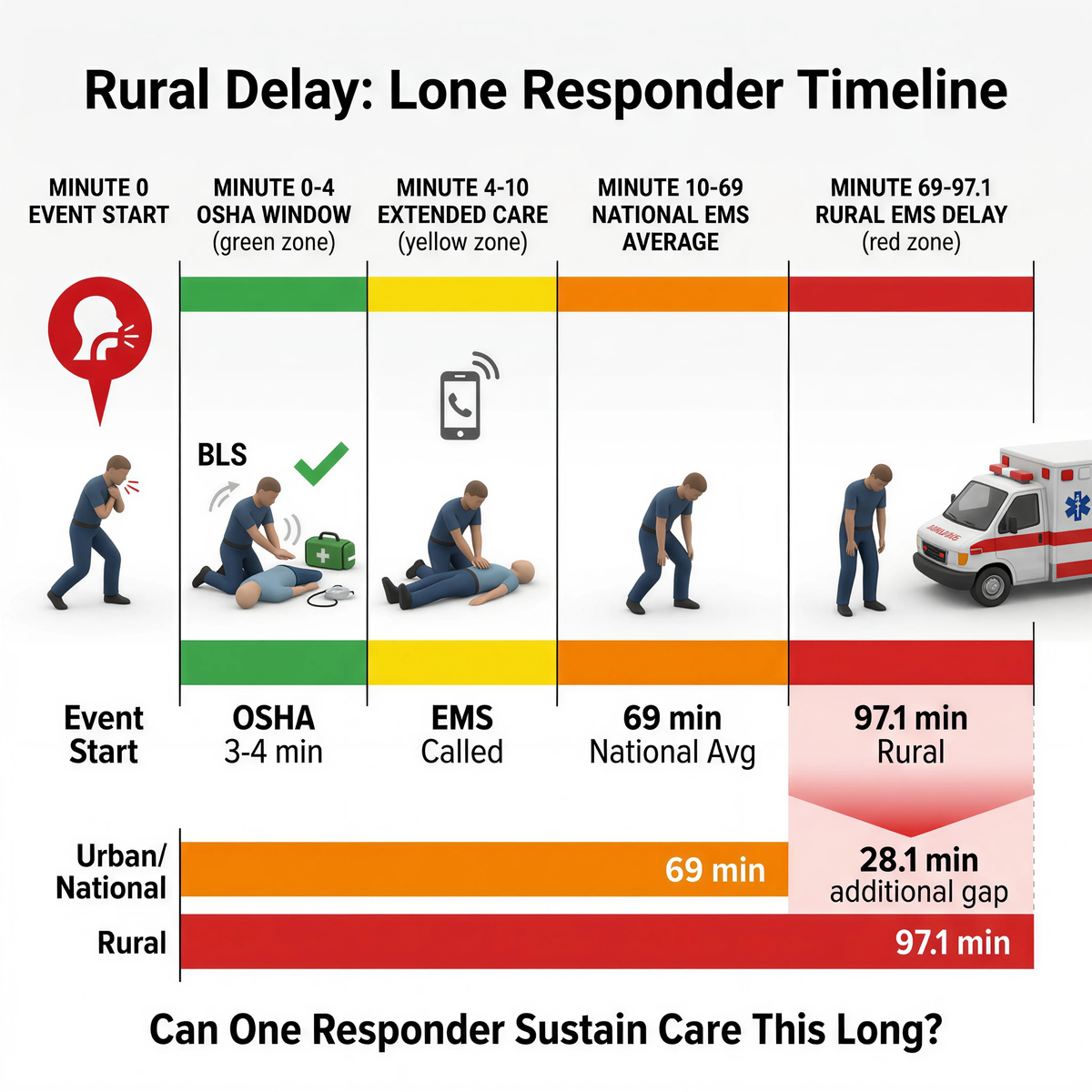
In remote transport and mobile work, airway failure often becomes a one-adult problem. OSHA still reads life-threatening first aid around a 3-4 minute window, while rural high-acuity EMS events average 97.1 minutes versus 69 minutes nationally. FDA's 2026 framework keeps suction devices in a narrow second-line role after failed BLS. One question decides the system: can one person recognize, act, retrieve, and hold the scene without breaking sequence? Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions. |
Most written response plans quietly assume another pair of hands will appear. A bus driver will have help. A yard lead will have another supervisor nearby. A route worker will have radio support that becomes physical support fast enough to matter. A remote depot will not leave one person carrying the whole event. A lot of rural and mobile operations do not work that way.
One adult may be the only responder in the scene. One adult may have to identify the event, begin first-line action, call for help, control bystanders, retrieve the backup layer, and stay with the person until EMS becomes real. OSHA's first-aid standard does not excuse that structure. If outside medical care is not in near proximity, the employer still has to ensure trained first aid and ready supplies at the worksite. In life-threatening events, OSHA has long interpreted that timing around 3 to 4 minutes.
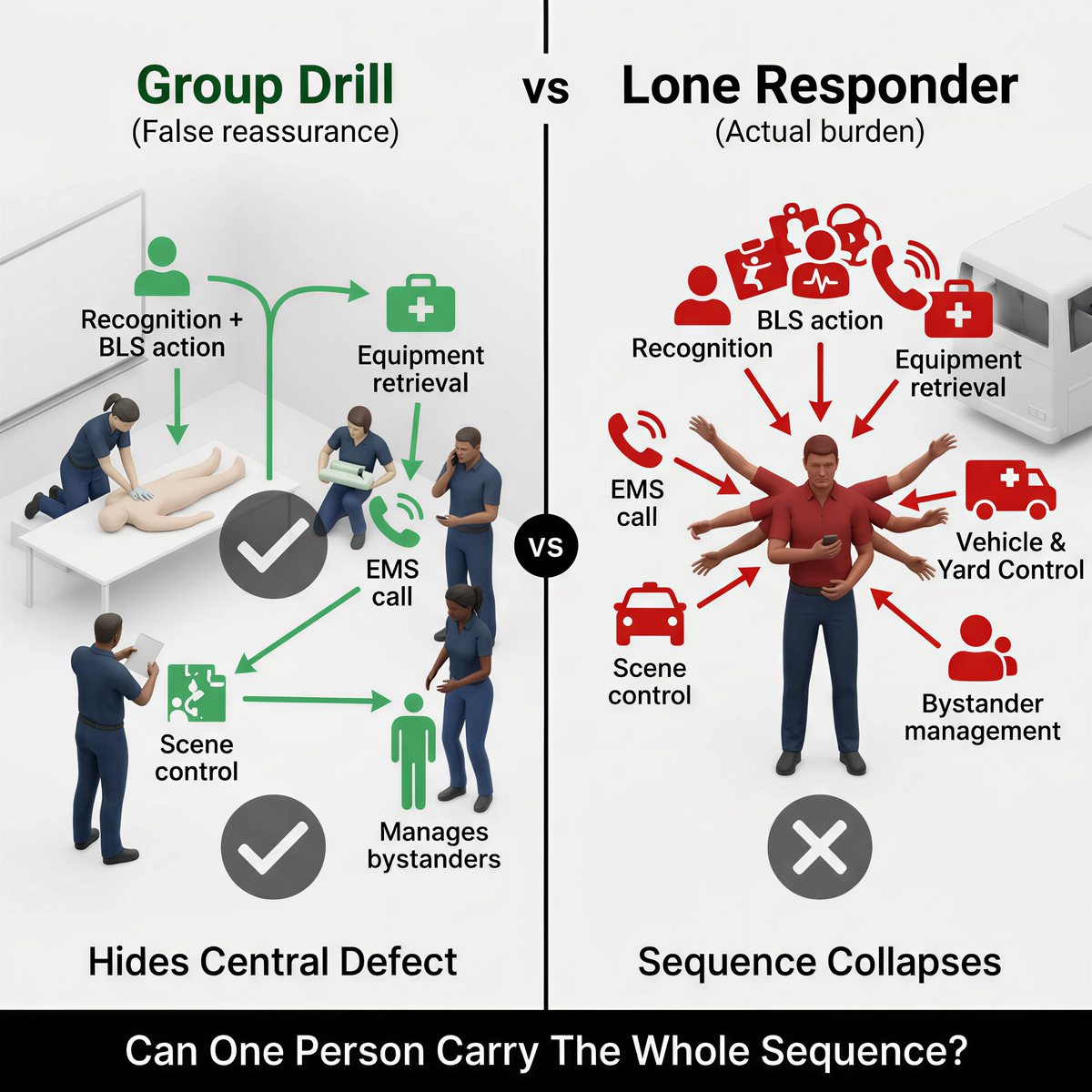
Group drills hide the central defect. One person calls. One person starts first-line action. One person retrieves equipment. One person opens the backup layer. The scenario looks organized because the training room supplied the missing hands. A lone responder does not get that luxury.
The sequence compresses into one body: recognition, first-line action, decision to escalate, retrieval, second-line use if first-line fails, scene control, EMS communication, and handoff. The training question is no longer whether staff received airway content. It becomes whether one adult can carry the sequence without collapsing it.
FDA's March 4, 2026 decision under DEN250012 sharpened that burden instead of reducing it. The category under 21 CFR 874.5400 is a 'suction anti-choking device as a second-line treatment' after unsuccessful use of a BLS choking protocol in complete airway obstruction. Retrieving, unpacking, or assembling the device before standard rescue can delay care. In lone-responder settings, the same person who should be starting first-line action may also be tempted to reach for the backup layer too early.
Generic compliance logs provide false reassurance: they prove content exposure but ignore the biomechanical load of a lone-responder environment.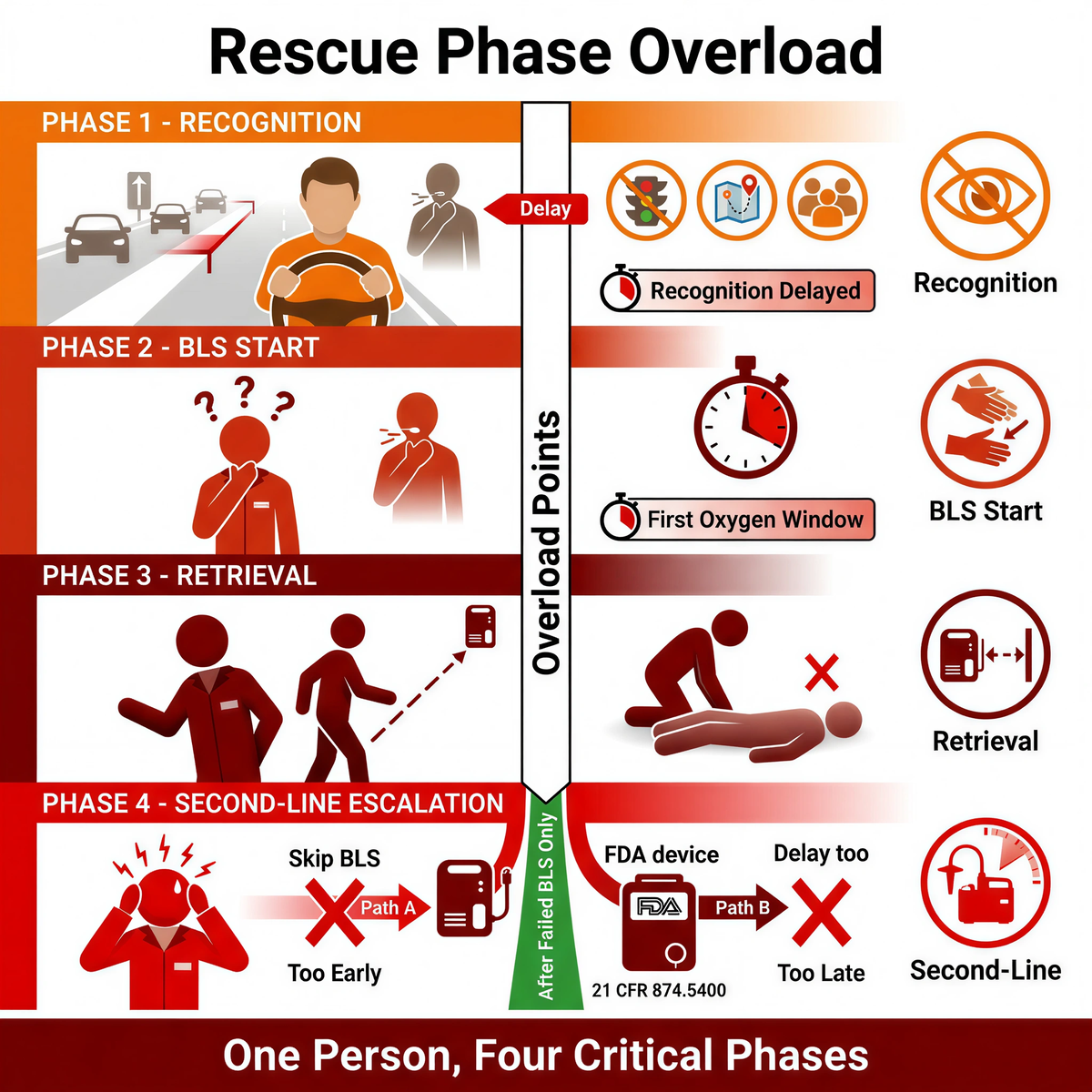
|
Rescue Phase |
Overload Risk |
Mitigation Strategy |
|
Recognition |
Driving, route monitoring, traffic, or yard supervision delay recognition of severe airway distress |
Train 'sentinel signals' for the actual environment instead of relying on textbook choking posture |
|
BLS start |
Hesitation and confirmation questions consume the first oxygen window |
Drill the AHA 2025 automated 5 back blows + 5 abdominal thrusts sequence until the first move is reflexive |
|
Retrieval |
Responder cannot leave the scene and fetch equipment without interrupting care |
Use asset mapping and route-specific staging so the backup layer can be reached without abandoning the patient |
|
Second-line escalation |
Pressure drives responders to skip or blur manual protocol boundaries |
Align training tightly with 21 CFR 874.5400 and QXN limits: second-line only after unsuccessful BLS |
The weak points repeat across buses, remote yards, field vehicles, and night-shift depots. The event is recognized too late because the responder is driving, spotting traffic, or supervising multiple people. First-line action starts late because the responder is still trying to understand what they are seeing. The backup layer is retrieved too early and disrupts BLS-first sequence, or too late because the responder cannot leave the scene immediately. EMS is called, but nobody has rehearsed what the responder keeps doing during the wait. Handoff becomes chaotic because the responder is still controlling the rest of the environment.
Fitiger's engineering and product safety view treats this as a role-overload problem, not a content problem. One person is carrying too many time-critical tasks inside too little time. The chain breaks where overload peaks.
This is not just a school bus problem. It shows up in rural yards, field vehicles, lone-operator routes, and small transfer points where one person is effectively the whole first-aid program. The bus environment simply exposes it faster. The driver may be the only adult. The aisle is narrow. The bus may still be moving when the event starts. The rider may be strapped in, seated away from the driver, or medically fragile in ways the route design never fully absorbed.
ACS reported in 2025 that rural high-acuity EMS activations averaged 97.1 minutes compared with 69 minutes nationally. That 28.1-minute gap does not describe the bus cabin itself. It does define the handoff reality once the route leaves the building. A lone responder may still be the active care system long after the call is placed.
|
Training Question |
Why It Matters In A Lone-Responder Scene |
|
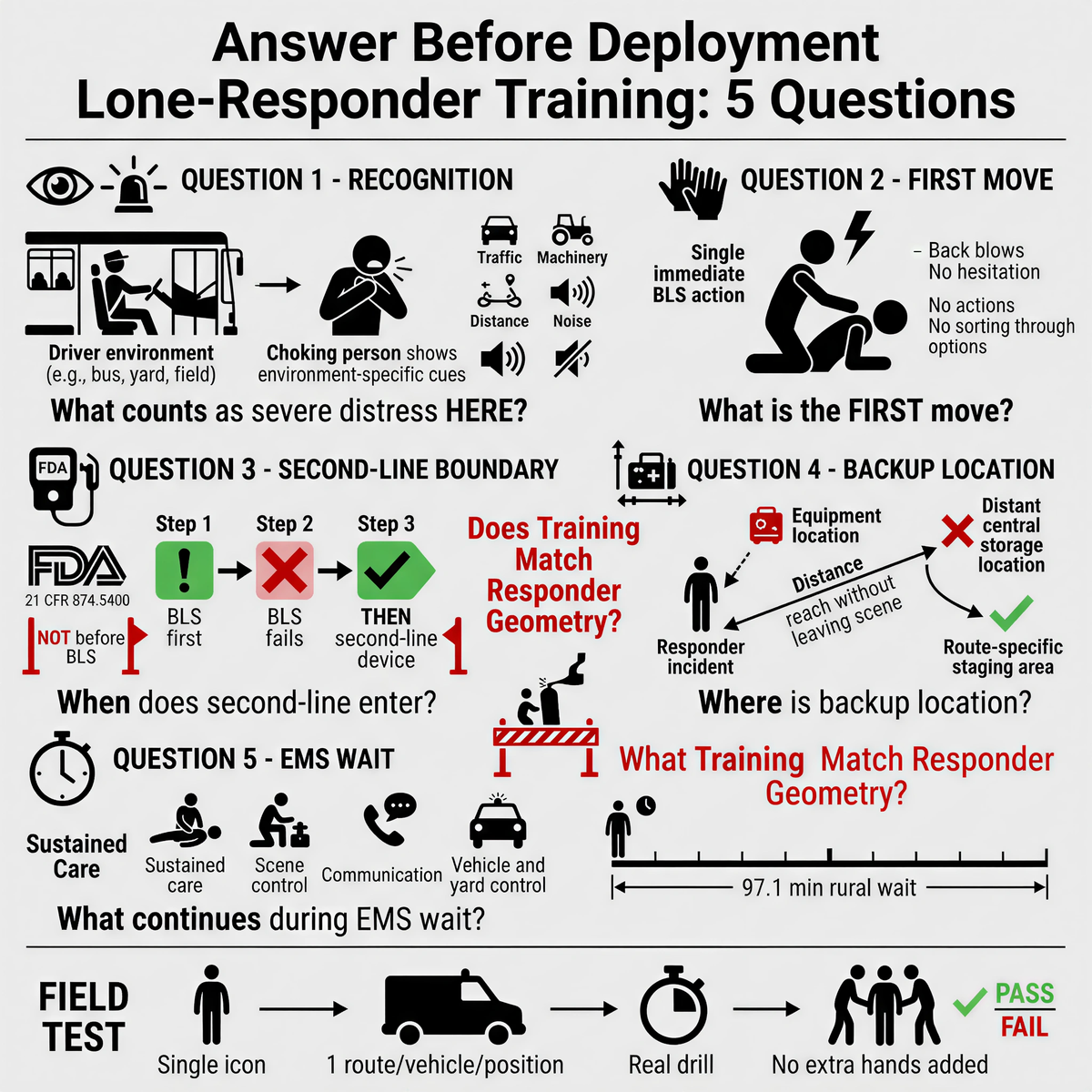
What counts as severe airway distress here? |
Drivers, yard staff, and route supervisors need cues that fit their environment, not abstract textbook posture alone. |
|
What is the first move? |
A single responder does not have time to sort through layered options while carrying the whole scene. |
|
When does second-line enter? |
The boundary has to stay aligned with DEN250012 / 21 CFR 874.5400: after unsuccessful BLS, not before. |
|
Where is the backup layer relative to the responder? |
Central storage fails when one person cannot leave the scene and return in time. |
|
What continues during the EMS wait? |
Rural delay forces the responder to sustain care, scene control, and communication at the same time. |
A stronger training file should show which roles are expected to respond first, which environments were drilled, which first-line sequence was trained, how second-line escalation is defined, where the backup layer is staged for that exact route or site, and what the responder is expected to do while waiting for EMS. The point is not training volume. The point is whether the training matches the responder geometry.
Managers usually look for the wrong fix first: another product, another cabinet, another policy sentence, another annual sign-off. Lone-responder systems rarely fail because they lacked one more object. They fail because one person was carrying a chain designed for three.
The right redesign questions are colder. Can the first adult in the scene recognize severe airway distress fast enough? Can that same person begin first-line action immediately? Can the backup layer be reached without abandoning the scene? Can the sequence hold if EMS is still far away? Can the responder sustain control of the vehicle, yard, passengers, or bystanders while doing all of that?
Pick one route, one vehicle, or one remote work position where one adult is likely to carry the whole event. Run one timed drill with that reality locked in: one responder, one incident point, one first-line sequence, one backup location, one EMS call. Do not add extra hands to make the drill look cleaner. If the sequence fails with one person, the real plan still has a hole.
Download the Remote & Mobile Readiness Toolkit
When help may be minutes away, readiness has to be planned before the emergency.
Download the Remote & Mobile Airway Safety Readiness Toolkit to map delays, assign roles, plan equipment access, and prepare your team for choking emergencies in rural, mobile, or field-based environments.
For a product-specific backup option, review the suction anti-choking device.
Why is lone-responder training different from ordinary first-aid training?
Because one person may have to recognize the event, start first-line action, retrieve the backup layer, call EMS, control the scene, and maintain care without another adult to split the sequence.
Does the FDA's 2026 second-line classification change first-line choking rescue?
No. Under DEN250012 / 21 CFR 874.5400, suction devices are second-line tools used only after unsuccessful BLS choking protocol in complete airway obstruction.
Why does rural EMS delay matter so much for lone responders?
Because high-acuity rural events average 97.1 minutes versus 69 minutes nationally. A lone responder may remain the active care system much longer than an urban plan assumes.
What should a good lone-responder drill measure?
It should measure recognition time, first-line start time, backup retrieval time, second-line readiness after failed BLS, and EMS handoff time in the actual route or work environment.
OSHA 29 CFR 1910.151 Medical services and first aid
OSHA 2007 near proximity interpretation
FDA safety communication, March 4, 2026
American College of Surgeons 2025 rural EMS study
This article is for education and operational planning only. It is not medical or legal advice. Follow current AHA or Red Cross choking-response guidance, applicable OSHA obligations, local policy, and emergency protocols. In a real emergency, call 911 or local emergency services immediately.




















