What matters first For a household checklist, see Fitiger's child and home choking safety readiness plan. |
Most choking-hazard articles read like refrigerator lists: grapes, hot dogs, popcorn, candy, nuts. The list helps, but it misses the part that changes the outcome. A choking hazard is not only a food. It is the collision between food shape, texture, bite size, chewing capacity, airway diameter, attention, posture, and supervision.
A whole grape can behave like a smooth plug in a toddler airway. A coin-cut hot dog can wedge because it is cylindrical, compressible, and close to airway diameter. A dense bread bolus can become dangerous in an older adult because saliva, dentition, chewing endurance, and swallow timing have changed. The same kitchen can contain three different risk maps depending on who is eating.
Prevention improves when families, schools, and care facilities stop asking only which foods are risky and start asking whether the food has been prepared for the person in front of them. Age matters. Development matters. Dentures matter. Dysphagia matters. So does the clock: once severe choking begins, the rescue window is measured in minutes.
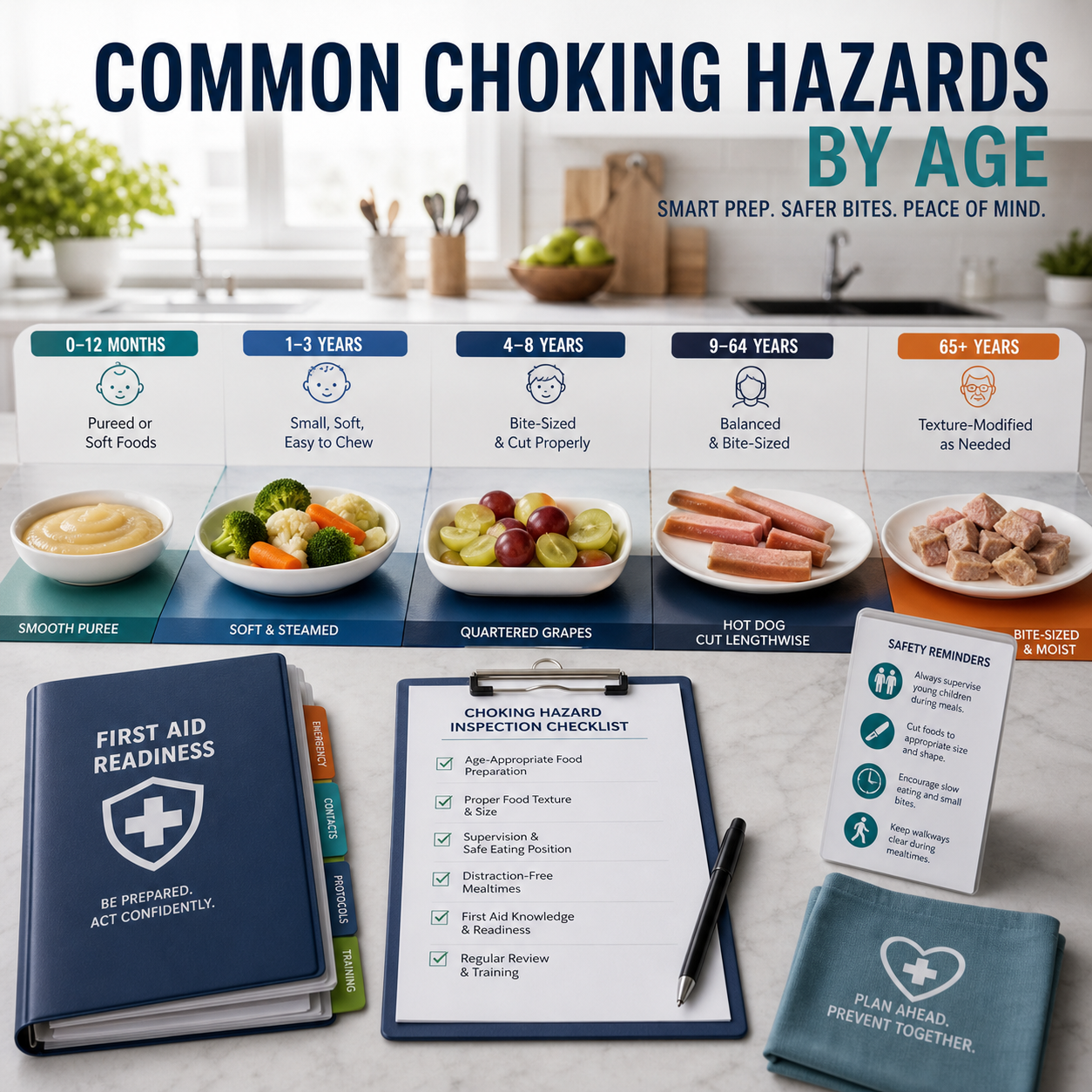
Age group | High-risk foods | Biological trigger | Biomechanical failure mode | Prevention priority |
Infant (0-1 year) | Whole grapes, hard pieces, chunks of raw fruit or vegetable, sticky nut butter, coin-sized objects | Immature chewing-swallow coordination; small airway; limited ability to self-clear | Food or object can enter the airway before coordinated chewing and swallow control mature | Use age-appropriate textures; avoid hard, round, sticky, or coin-sized foods; follow pediatric guidance |
Toddler / preschool (1-4 years) | Hot dogs, whole grapes, popcorn, hard candy, nuts, seeds, marshmallows, large raw vegetables | Exploratory eating, talking while chewing, incomplete molar grinding, fast movement | Round or compressible foods can seal the airway plug-style; sticky foods can adhere and resist clearing | Quarter grapes lengthwise; cut hot dogs lengthwise, then small; avoid popcorn, nuts, hard candy, and thick sticky globs |
School-age child | Hot dogs, grapes, candy, popcorn, large meat chunks, food challenges, rushed cafeteria foods | Distraction, laughing, talking, running, peer dares, short lunch periods | A preventable bite-size problem turns into severe obstruction when supervision and meal pace fail | Seat children while eating; prohibit food dares; slow meal timing; train staff on 2025 choking sequence |
Adult | Large meat pieces, steak, bread bolus, poorly chewed food, alcohol-associated meals | Speed, distraction, impaired coordination, poor chewing, large bites | Dense bolus lodges when bite size and swallowing coordination fail | Cut dense foods; avoid rushed eating; maintain first-aid readiness in dining areas |
Senior (65+) | Dry meat, dense bread, poorly cut solids, pills, mixed textures, sticky foods, poorly fitted dentures | Lower swallow reserve, tooth loss, dentures, dry mouth, dysphagia, fatigue | Risk shifts from shape to stamina: chewing fatigue and bolus adhesion define the failure zone | Texture modification, supervision, swallow plans, hydration, denture fit checks, and response staging |
Infants are not small toddlers. Their oral control, airway size, posture control, and cough effectiveness are still developing. The danger is not only a classic choking plug. Food can enter the airway quietly when coordination fails, especially in children with feeding disorders, neurologic impairment, airway abnormalities, or delayed development.

Pediatric aspiration can be silent. One large pediatric study reported that thin fluids were silently aspirated in 81% of patients who silently aspirated, and research on feeding difficulties has repeatedly shown that children with neurologic problems are at higher risk. Silent risk is the reason 'no dramatic coughing' should never be treated as proof of safety in medically complex children.
For infants, the prevention rule is strict: use developmentally appropriate textures, avoid hard or round foods, never offer coin-shaped pieces, and supervise eating from close range. Thick globs of nut butter deserve special caution. They do not behave like a loose crumb. A sticky bolus can smear, adhere, and seal like a high-friction plug rather than breaking apart cleanly.
Infant food or object | Why it becomes dangerous | Safer handling |
Whole grapes / round fruit pieces | Smooth round geometry can block a small airway without crumbling | Avoid whole grapes; use age-appropriate soft textures only when developmentally ready |
Hard raw vegetable chunks | Requires chewing strength and coordinated grinding the infant does not have | Cook until soft and prepare in pediatrician-approved texture |
Thick nut butter glob | Sticky mass can adhere to the mouth, palate, or airway and resist movement | Use only when age-appropriate, thinned/spread very thinly, and medically safe for the child |
Coins, beads, small toy parts | Non-food object can enter airway during mouthing behavior | Keep small objects outside reach; use the small-parts tube logic for home and daycare audits |
Engineering analysis identifies round, compressible shapes as efficient biological plugs for the pediatric airway. The American Academy of Pediatrics has long singled out hot dogs as the food most commonly associated with fatal choking among children. The shape explains the risk: a hot dog slice is cylindrical, soft enough to compress, and close enough to airway diameter to wedge tightly instead of fragmenting.

Grapes create a different version of the same problem. They are smooth, wet, and round. When swallowed whole or cut into round halves, they can slide into the airway and seal. The safer cut is lengthwise quarters for young children, with size adjusted for maturity and local policy.
Popcorn, hard candy, nuts, and seeds add another risk. They are small enough to inhale, hard enough to resist chewing, and easy to eat while walking, laughing, or playing. These foods are poor matches for toddlers because the eating behavior is still being learned while the airway remains small.
Toddler hazard | Failure mode | Better preparation or policy |
Hot dogs | Cylindrical, compressible plug; high association with fatal pediatric choking | Cut lengthwise first, then into small irregular pieces; avoid coin-cut rounds |
Whole grapes / cherry tomatoes | Smooth sphere can seal the airway | Quarter lengthwise; never serve whole to young children |
Popcorn | Irregular hard pieces and light fragments can be inhaled | Avoid in children under 4 or until developmentally safe |
Hard candy / gum | Hard or sticky material resists chewing and can lodge suddenly | Avoid in young children |
Nuts and seeds | Small hard pieces can be inhaled during immature chewing | Avoid or use medically appropriate alternatives |
Sticky nut butter | Adhesive bolus can coat and obstruct instead of clearing cleanly | Spread thinly; never serve in spoonfuls |
School-age children usually have better chewing ability than toddlers. Cafeteria risk does not disappear. It changes shape. A child who can safely chew a food at home may become unsafe when lunch is rushed, table noise is high, peers are laughing, or a food challenge starts. The airway risk moves from pure anatomy toward behavior and supervision.

Schools should treat choking prevention as a cafeteria design problem. Children need enough seated time to eat, adults close enough to recognize silence, and rules that stop running, laughing with food, stuffing contests, and dares. A food policy without lunchroom behavior control is only half a prevention system.
For severe choking in conscious children, the 2025 AHA/AAP guidance recommends repeated cycles of 5 back blows alternating with 5 abdominal thrusts until the object is expelled or the child becomes unresponsive. Staff trained on older abdominal-thrust-only language need a refresh.
Cafeteria variable | Why it increases choking risk | Operational control |
Short lunch period | Children take larger bites and swallow before chewing fully | Protect seated eating time; avoid rushing dismissal |
High noise | Silent choking is easier to miss | Assign adult sight lines and zones |
Peer dares / food challenges | Encourages stuffing and unsafe bite sizes | Explicit prohibition and staff enforcement |
Walking while eating | Posture and distraction increase airway risk | Food stays at tables |
Untrained monitors | Recognition and first action are delayed | Train lunchroom staff, substitutes, and after-school staff |
Healthy adults choke less often than young children and older adults, but adult events can be severe because the obstructing food is often dense: steak, meat chunks, bread bolus, or poorly chewed mixed textures. Alcohol, distraction, dental problems, neurologic disease, and eating alone can remove the margin that normally keeps swallowing safe.
The prevention pattern is not complicated. Cut dense foods before serving. Slow the meal. Avoid talking or laughing with a large bite in the mouth. Keep first-aid knowledge current in restaurants, workplaces, churches, community centers, and homes where older relatives eat.
For geriatric populations, risk migrates from shape to stamina: chewing fatigue and bolus adhesion define the failure zone. A food that looks soft on a plate can become dangerous after poor chewing, low saliva, loose dentures, delayed swallow initiation, or dysphagia. Dense bread can behave like a sponge after moisture exposure, swelling and forming a cohesive bolus that does not clear easily.

The age signal is not subtle. A swallowing and frailty review notes that people over 65 have seven times higher risk for choking on food than children aged 1-4. That makes elder-care meal planning a safety intervention, not a hospitality detail.
Texture matters because clearance pressure is not the same across foods. Mechanical simulation work found that clearing an example starch-based bolus required 5.4 kPa, compared with 1.7 kPa for a gum-based sample of equal apparent viscosity. In practical terms, some soft-looking foods can be mechanically harder to clear than they look.
Senior hazard | Failure mode | Control |
Dry meat / steak | Requires sustained chewing and strong bolus control | Moisten, mince, shred, or avoid depending on swallow plan |
Dense white bread / bread bolus | Absorbs moisture, swells, and forms a cohesive mass | Serve with moisture, smaller portions, or texture-modified alternatives |
Pills | Can lodge during dry swallow or impaired coordination | Medication review; safe administration plan; do not crush unless authorized |
Mixed textures | Liquid and solids separate during swallow, increasing timing demands | Use speech-language pathology guidance for dysphagia diets |
Poorly fitted dentures | Reduces chewing effectiveness and bolus control | Denture-fit review and supervised mealtime when needed |
Sticky foods | Adhere to palate or oral surfaces, increasing residue | Thin, modify, or avoid according to individual swallow tolerance |
A food list gives a starting point. It cannot replace a person-specific risk check. The safer question set is direct: who is eating, what is the exact texture, how large is the bite, what is the supervision level, what is the swallow condition, and what happens if the first rescue attempt fails?

This is where Fitiger's engineering and product safety work sits. A stronger prevention culture should reduce the number of moments when a second-line device is ever needed. QXN suction anti-choking devices, under 21 CFR 874.5400, are FDA-authorized as second-line treatment after unsuccessful basic life support choking protocol steps. They are not a license to serve unsafe food, skip supervision, or delay manual rescue.
A second-line backup device belongs after first-line failure, staged close enough that the oxygen window is not wasted on retrieval.
Layer | What it controls | Examples |
Prevention | Keeps the bolus from becoming an airway plug | Age-specific food prep, seated eating, texture modification, denture checks |
Recognition | Reduces delay when the airway is blocked | No cough, no voice, panic, hands to throat, color change, sudden silence |
First-line rescue | Uses current manual protocol immediately | 2025 child/adult cycles: 5 back blows + 5 abdominal thrusts; infant cycles: 5 back blows + 5 chest thrusts |
Second-line redundancy | Adds a backup pathway after unsuccessful BLS choking protocol steps | FDA-authorized QXN suction anti-choking device where policy and labeling support use |
Post-incident review | Turns the event into prevention data | Food type, bite size, location, staffing, response latency, EMS, follow-up |
For infants: keep foods developmentally appropriate, avoid hard and round pieces, supervise closely, and ask a pediatric clinician or feeding specialist when swallowing concerns exist.
For toddlers and preschoolers: remove or modify hot dogs, grapes, hard candy, popcorn, nuts, seeds, marshmallows, raw vegetable chunks, and spoonfuls of sticky nut butter. Shape modification matters as much as size reduction.
For schools: slow the cafeteria, keep children seated while eating, enforce no food dares, train lunchroom adults on severe choking recognition, and update staff on the 2025 AHA/AAP sequence.
For adults: cut dense foods, avoid rushed eating, limit distraction during large bites, and maintain first-aid readiness in group dining spaces.
For older adults: use texture plans, monitor denture fit, address dry mouth and dysphagia, modify bread and meat textures, and supervise high-risk meals without turning dining into a rushed task.
Hot dogs are the food most commonly associated with fatal choking among children. Their cylindrical, compressible shape can fit the airway like a plug. Whole grapes, hard candy, nuts, popcorn, and sticky foods also require strict age-specific modification or avoidance.
Older adults may have reduced chewing strength, tooth loss, dentures, dry mouth, dysphagia, neurologic disease, and lower swallow reserve. Research notes that people over 65 have about seven times higher risk for choking on food than children aged 1-4.
No. Size helps, but shape, texture, stickiness, supervision, posture, swallow ability, and behavior all matter. A small sticky bolus or dense bread mass can still be dangerous if it adheres, swells, or resists clearance.
It does not replace prevention or first-line rescue. Under 21 CFR 874.5400, a QXN suction anti-choking device is a second-line treatment after unsuccessful basic life support choking protocol steps. Food preparation, supervision, and age-correct rescue remain first.
American Academy of Pediatrics - Supports pediatric choking hazard categories, hot dog fatal-risk language, and age-based prevention framing. Full link
HealthyChildren.org / AAP - Supports practical food avoidance and modification recommendations for young children. Full link
Cichero - Supports the seven-times-higher food choking risk in people over 65 compared with children aged 1-4 and the elder-care texture-modification rationale. Full link
Velayutham et al. - Supports pediatric silent aspiration statistics, including thin fluids silently aspirated in 81% of the relevant patient group. Full link
Redfearn et al. - Supports 5.4 kPa vs 1.7 kPa bolus-clearing pressure comparison for starch-based vs gum-based samples. Full link
AHA Newsroom - Supports 2025 choking sequence updates for children/adults and infants. Full link
FDA De Novo Database - Supports FDA authorization, regulation number 874.5400, product code QXN, decision date, and second-line treatment identity. Full link
FDA TPLC Product Code QXN - Supports QXN device definition, Class II status, and second-line use after unsuccessful BLS choking protocol. Full link
This article is for education, emergency preparedness planning, and product-safety discussion. It is not medical advice, diagnosis, treatment, legal advice, or a substitute for CPR/first-aid training. Follow pediatrician guidance, speech-language pathology recommendations, care plans, school policy, local emergency protocols, and current first-aid training. In a choking emergency, call 911 or local emergency services and follow established choking rescue protocols.




















