Key Takeaway |
|
A post-incident file should show four things clearly: what happened, what was tried first, when the backup layer entered the sequence, and how long the team functioned before EMS took over. In rural and mobile settings, those details are not paperwork. They are the only reliable record of whether the response chain actually worked. |
Incident records function as evidence: they transform the biological chaos of hypoxia into auditable operational data.
A severe airway event in a school bus, rural fleet, yard, or remote route usually unfolds inside confusion, motion, noise, and incomplete memory. People remember the shock of it. They do not all remember the sequence the same way. One responder will swear the backup layer was retrieved immediately. Another will remember delay. Someone will think EMS arrived fast. The clock will say otherwise.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
A usable post-incident file turns that fog into something the team can actually learn from.
For any event involving a suction anti-choking device, the regulatory boundary is already clear. FDA’s March 4, 2026 De Novo order DEN250012 created 21 CFR 874.5400 for a 'suction anti-choking device as a second-line treatment' after unsuccessful use of a BLS choking protocol in complete airway obstruction. A serious incident file has to show what happened before the backup layer was used, not just whether the backup layer was used.
|
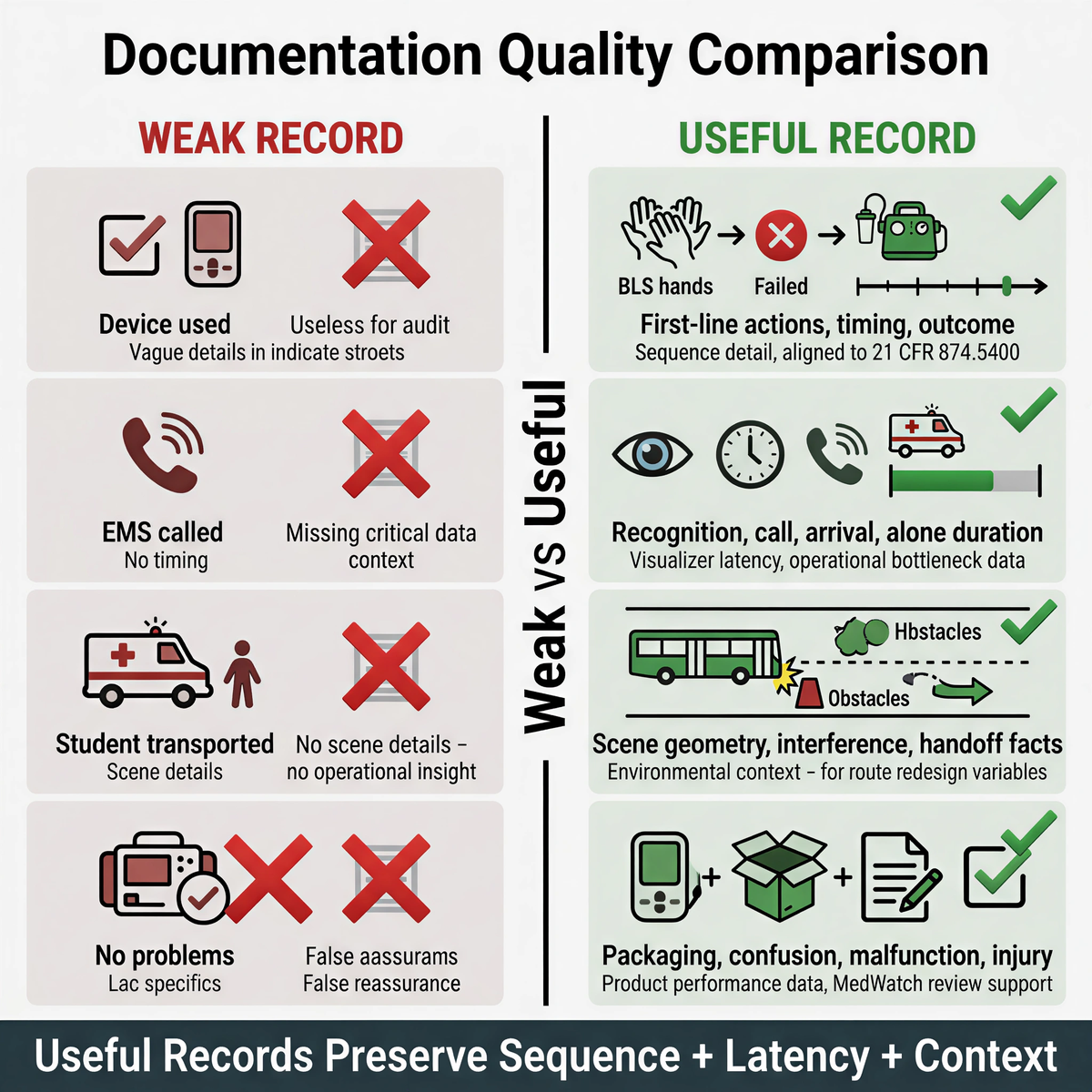
Weak Record |
Useful Record |
|
Device used |
First-line actions attempted before suction; time second-line entered the sequence; immediate outcome. |
|
EMS called. |
Recognition time, 911 call time, arrival time, and duration the responder was functionally alone. |
|
Student transported. |
Scene geometry, stop conditions, aisle or tiedown interference, and handoff facts. |
|
No problems with equipment. |
Packaging behavior, user confusion, malfunction, visible injury, and product quality observations. |
A weak record says 'Device used.' A useful record says what the responder first saw, when severe airway distress was recognized, what first-line measures were attempted, whether those measures failed or were incomplete, when the backup layer entered the sequence, what happened immediately after that, and when EMS became real.
Rural and mobile events usually fail on delay long before they fail on intent. The person in distress may be functionally alone for longer than anyone in the scene realizes. ACS reported in 2025 that rural total EMS call times were almost 20 minutes longer than the national average, and that high-acuity rural activations averaged 97.1 minutes compared with 69 minutes nationally. A post-incident review that does not capture how long the team carried the event before handoff misses the central engineering problem.
For Fitiger, the post-incident audit still follows the same four-link chain: recognition latency, retrieval latency,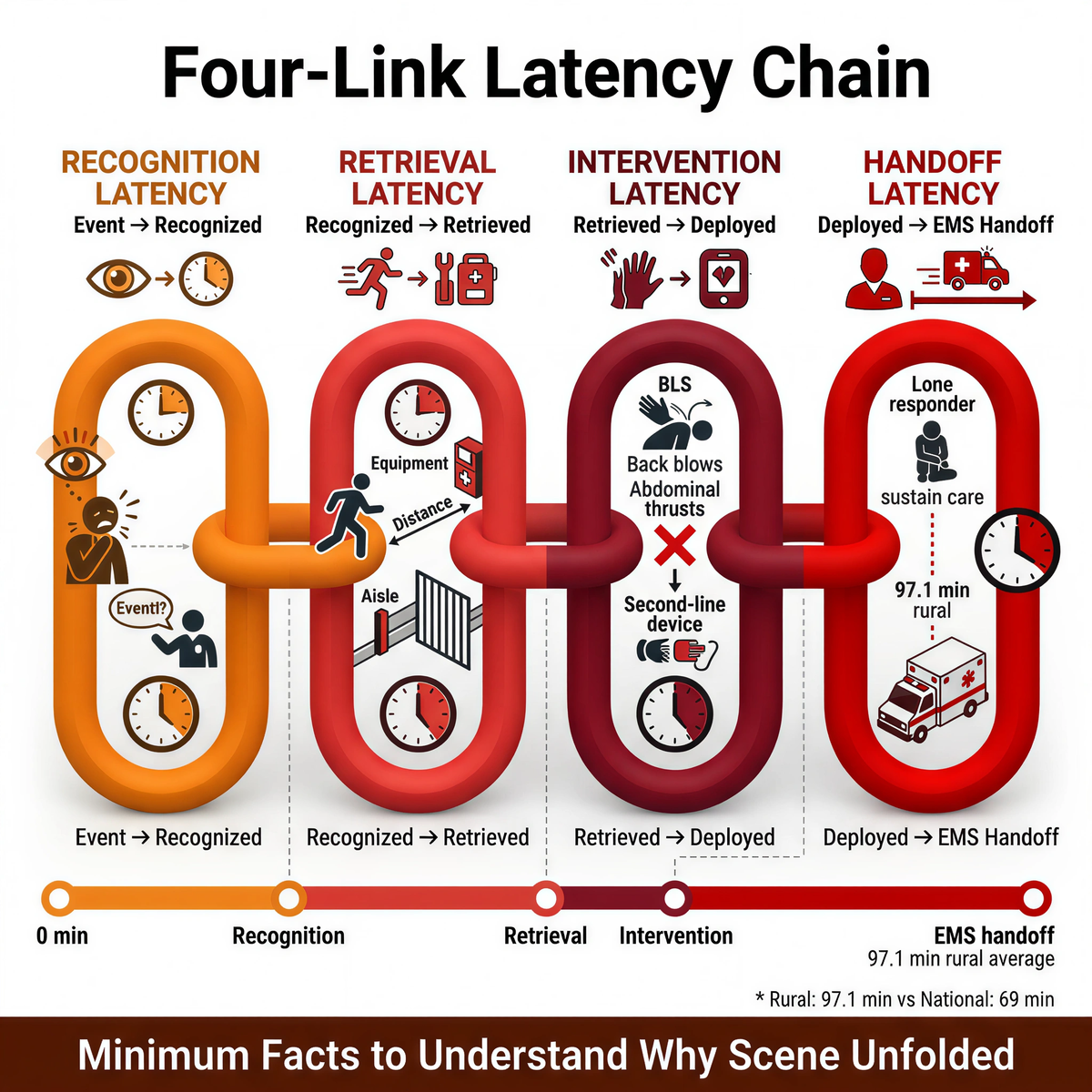
intervention latency, and handoff latency. Those are the minimum facts needed to understand why the scene unfolded the way it did.
|
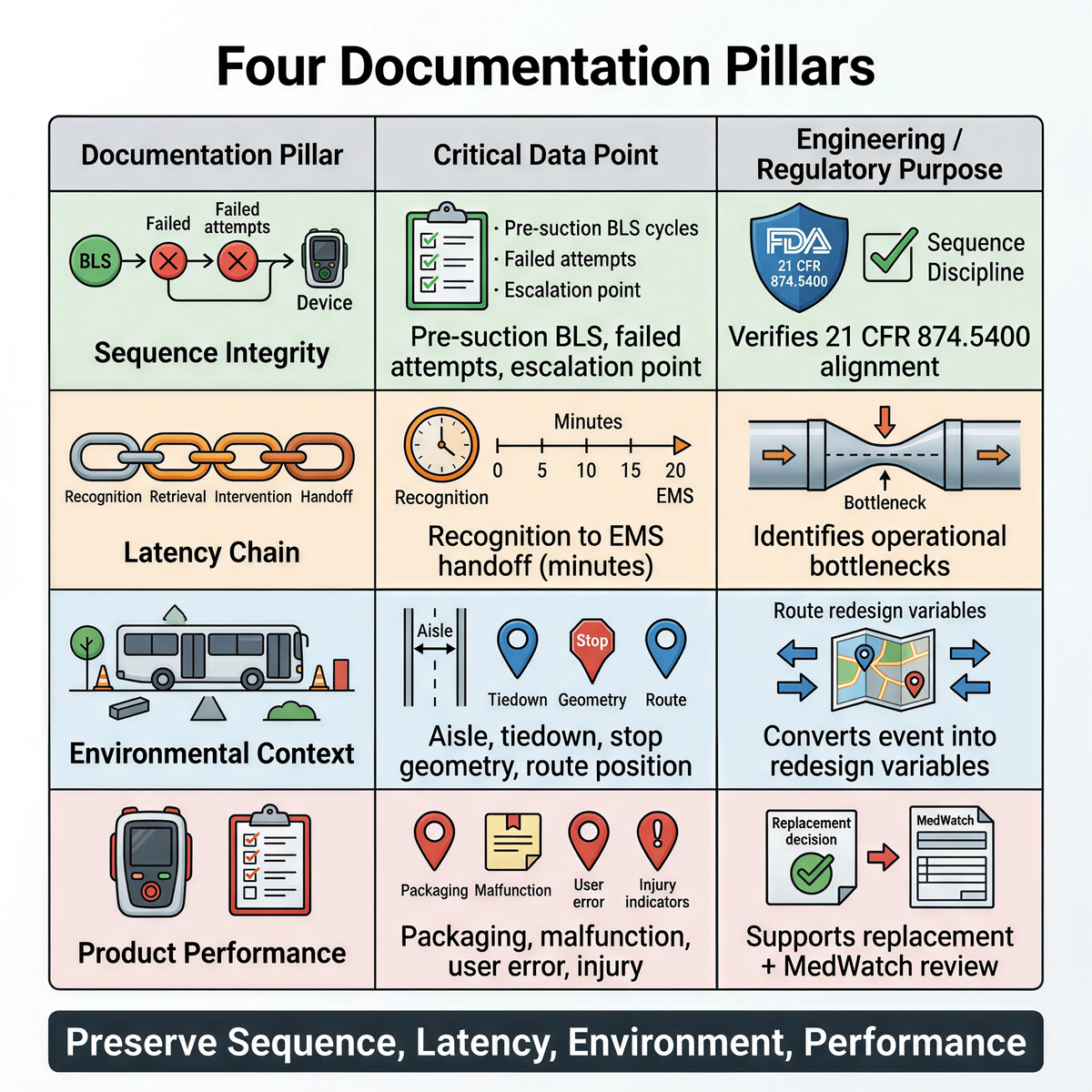
Documentation Pillar |
Critical Data Point |
Engineering / Regulatory Purpose |
|
Sequence Integrity |
Pre-suction BLS cycles, failed manual attempts, point of escalation |
Verifies alignment with 21 CFR 874.5400 and protects sequence discipline |
|
Latency Chain |
Recognition to EMS handoff in minutes |
Identifies operational bottlenecks inside the first useful window |
|
Environmental Context |
Aisle width, tiedown interference, stop geometry, route position |
Converts the event into route and vehicle redesign variables |
|
Product Performance |
Packaging friction, malfunction, user-error notes, visible injury |
Supports replacement decisions and feeds voluntary MedWatch review |
A classroom, a bus, a loading lane, a yard perimeter, and a remote route shoulder are not interchangeable scenes. The same event can succeed in one and fail in another because the physical setting changes leverage, reach, communication, and control.
For school transportation the file should note whether the bus was moving when the event started, whether an aide was present, where the rider was seated, whether restraints, tiedowns, or aisle width slowed access, whether pulling over added delay, and whether other students complicated the response. For rural fleets and depots, the file should note the exact incident point, distance to the nearest first-aid resources, whether the responder was alone, whether gates, traffic, or equipment blocked access, and whether route position changed the EMS wait materially.
Environmental details are diagnostic: they convert a traumatic event into a route-redesign variable.
If a second-line device was involved, the team should record the exact product used, whether the unit appeared intact before use, whether the packaging opened as expected, whether any component failed, stuck, leaked, or behaved unexpectedly, whether visible injury occurred during or after use, whether the responder reported confusion about operation, and whether the device appeared to function as designed.
FDA reporting rules are not the same for every setting. A school nurse office is not considered a 'device user facility' for mandatory Medical Device Reporting, and FDA guidance says user facilities do not include school nurse offices or employee health units. That means most school transportation teams are not sitting inside the mandatory user-facility MDR lane by default.
That does not mean the event should disappear into an internal memo. FDA’s MedWatch system remains available for voluntary reporting by health professionals, consumers, and patients for serious adverse events, product quality problems, product use errors, and device-related concerns. If a district, fleet, nurse, or safety team sees a serious device problem, an unexpected malfunction, a meaningful product quality defect, or an injury pattern worth flagging, that should be evaluated for MedWatch reporting.
A practical internal protocol should answer three plain questions: who decides whether voluntary FDA reporting is considered, what facts must be gathered before that decision, and where the final report, if filed, will be stored.
Post-incident governance usually fails at handoff. Transportation assumes the nurse owns the review. The nurse assumes transportation owns the route facts. Safety assumes procurement owns the device record. Procurement keeps the invoice and nothing else. A month later, nobody owns the event.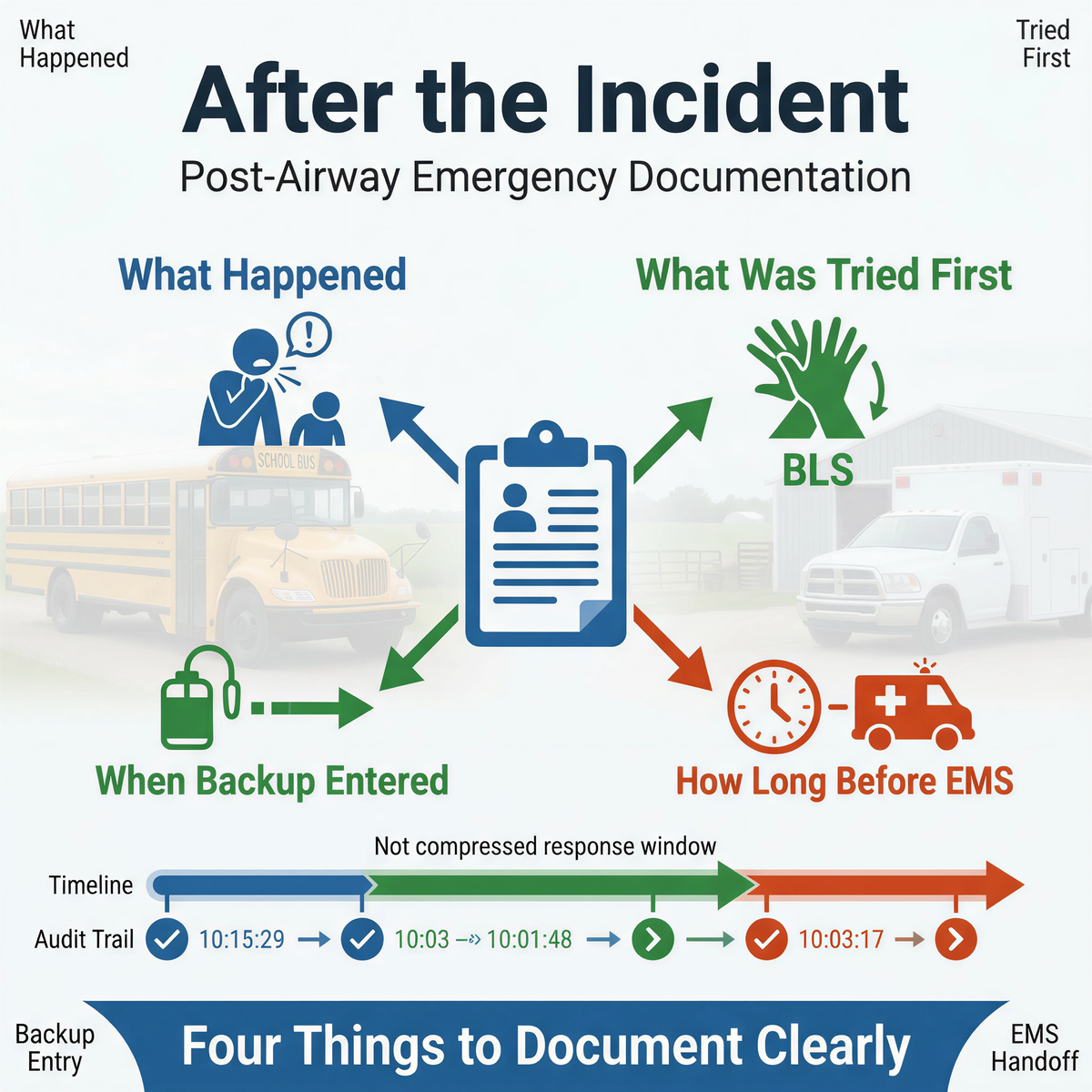
A strong post-incident system names the owner for each piece: route facts owner, training record owner, equipment inspection owner, EMS handoff record owner, after-action review owner, and voluntary FDA reporting decision owner, if applicable. That list looks administrative. It is operational. A review without ownership turns into memory drift.
For school transportation and rural fleets, the after-action review should end with a short decision file: what failed first, what delayed the scene most, what part of the route or site layout made that delay possible, whether staffing, placement, or training needs to change, whether the same problem could happen again tomorrow, who is responsible for fixing it, and by when.
A school bus event may reveal that the nurse office is irrelevant once the bus leaves campus. A rural yard event may reveal that central storage is not coverage. A fleet incident may reveal that one responder cannot carry both first-line action and backup retrieval without breaking sequence. A device issue may reveal that the product needs inspection, replacement, or outside reporting.
It should preserve sequence integrity, latency data, environmental context, and product performance so the team can reconstruct what happened and redesign the weak point.
School nurse offices are not device user facilities for mandatory MDR by default, but serious product concerns can still be evaluated for voluntary MedWatch reporting.
Because rural EMS high-acuity calls averaged 97.1 minutes versus 69 minutes nationally in ACS 2025 data, so the team may carry the scene much longer than expected.
Because 21 CFR 874.5400 defines the device as second-line after unsuccessful BLS choking protocol, so the file must show first-line actions before escalation.
FDA MedWatch voluntary reporting page
FDA MDR guidance / user facilities
American College of Surgeons 2025 rural EMS study press release
This article is for educational and operational planning purposes only. It does not provide medical or legal advice. Always follow current AHA or Red Cross choking-response guidance, applicable workplace and school policies, and local EMS procedures. In a real emergency, activate emergency medical services immediately and begin trained first-line response without delay.




















