Alyssa's Law was not written as a choking law. It was written to shorten emergency notification time in schools through silent panic alert systems that connect staff to law enforcement and first responders. In 2026, that matters for airway safety too. Once a school can trigger a silent alert, identify where it came from, and move the right people toward the right room without delay, the same infrastructure starts helping with choking, collapse, allergic reactions, and other medical emergencies that punish hesitation.

Alyssa's Law changes airway safety indirectly but meaningfully. It pushes schools to install faster alert systems, clearer location-aware workflows, and more reliable communication paths. Manual first aid still comes first. The difference is that the responder no longer has to leave the scene to find help or explain where the emergency is happening. The system starts moving with them.
The old school emergency model depended on fixed phones, front offices, wall stations, radios, or somebody running into the hallway to get help. That may be enough in a drill. It breaks down fast in a real medical event.
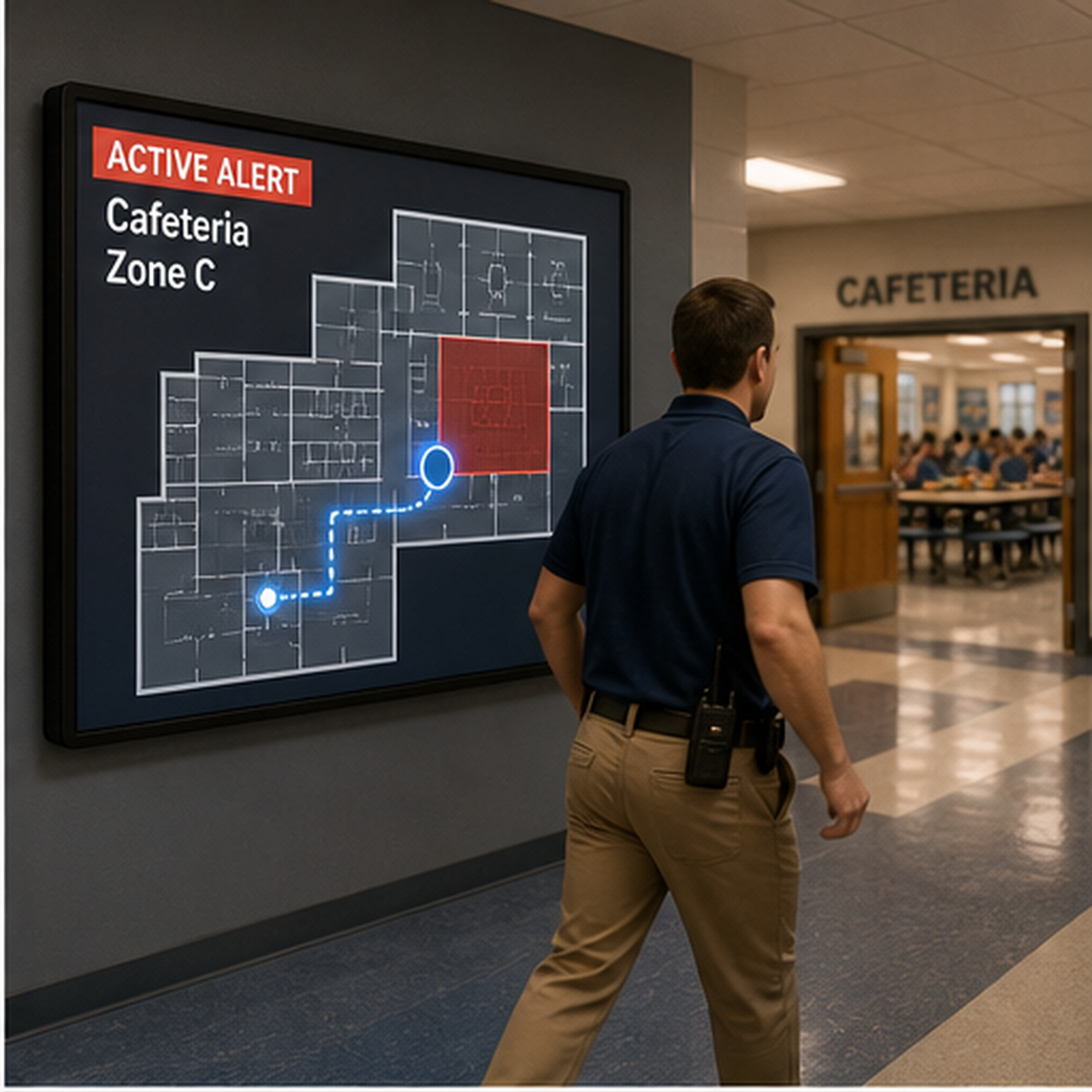
Picture a noisy lunchroom. A student stands up suddenly, stops talking, and can't cough. One adult starts moving in. Another reaches for a phone. A third tries to wave down help from across the room. Nothing about that scene feels organized at first. The first minute gets eaten by uncertainty.
Silent alert infrastructure bridges the critical gap in these high-decibel environments. The responder who begins back blows or abdominal thrusts should not also be the one leaving the child to hunt for a phone or explain which room needs help.
New Jersey's Alyssa's Law requires public elementary and secondary school buildings to be equipped with panic alarms or emergency mechanisms directly linked to law enforcement. Texas went further with S.B. 838, requiring each classroom in a school district or open-enrollment charter school to have silent panic alert technology that allows immediate contact with school emergency services, law enforcement, health departments, and fire departments. Texas also requires location to be included with an alert.
None of those laws say, 'This is a choking statute.' They don't have to. They are changing the built response environment inside schools. Once that environment exists, it stops being useful only for lockdowns. It becomes part of the medical response chain too.

Severe choking is a first-minute emergency. Current American Heart Association guidance for a conscious child with severe foreign-body airway obstruction is repeated cycles of 5 back blows followed by 5 abdominal thrusts until the object is expelled or the child becomes unresponsive. If the child becomes unresponsive, CPR begins, and only a visible object should be removed from the mouth. The sequence is straightforward. The harder part, in many schools, is everything around it: who is called, who brings backup equipment, who clears the path, and who knows exactly where the event is happening.
By shortening the notification arc, Alyssa's Law systems directly support the first-minute rescue window. They do not replace first aid. They reduce the communication gap around first aid. The responder can stay with the student. The school nurse, administrator, security officer, or trained staff member can start moving. If the school's alert system includes location, the response starts toward a room instead of toward a guess.

The phrase 'panic alarm' sounds simple. In practice, the value is bigger than the button.
A useful school emergency system now has to do more than fire off a generic notification. It has to sort who needs to know, what kind of emergency this is, and where to send people. Silent panic alert technology in current school safety guidance is no longer just an alarm. It is response infrastructure.
For choking events, this changes the whole shape of the first minute. The teacher doesn't have to choose between helping and reporting. The system can handle reporting while the teacher keeps both hands in the scene.
A lot of school safety planning still imagines medical response as something the nurse handles. That assumption is fragile.
Not every campus has a full-time nurse in the building at every moment. Not every student emergency happens in the nurse's office. Many happen in cafeterias, hallways, classrooms, gyms, buses, after-school programs, and transitional spaces where the nearest adult is not a clinician. That means the true first responder is often a teacher, aide, coach, monitor, or administrator.
Alyssa's Law infrastructure helps schools adapt to that reality. It does not create medical expertise. It compensates for delay. It turns nearby adults into connected responders instead of isolated witnesses.
Manual first aid remains the first line. In the current U.S. regulatory framework, suction anti-choking devices sit in a different place. FDA's March 4, 2026 De Novo decision for product code QXN established this category as Class II and defined it as a suction anti-choking device used as a second-line treatment after unsuccessful use of a basic life support choking protocol.
A second-line backup should never delay the 5-and-5 sequence. It should never replace accredited training. It should be staged as a controlled backup layer in schools that are building a broader response system.
The practical takeaway is not that every panic system automatically solves medical emergencies. Plenty of systems still create noise without creating speed.
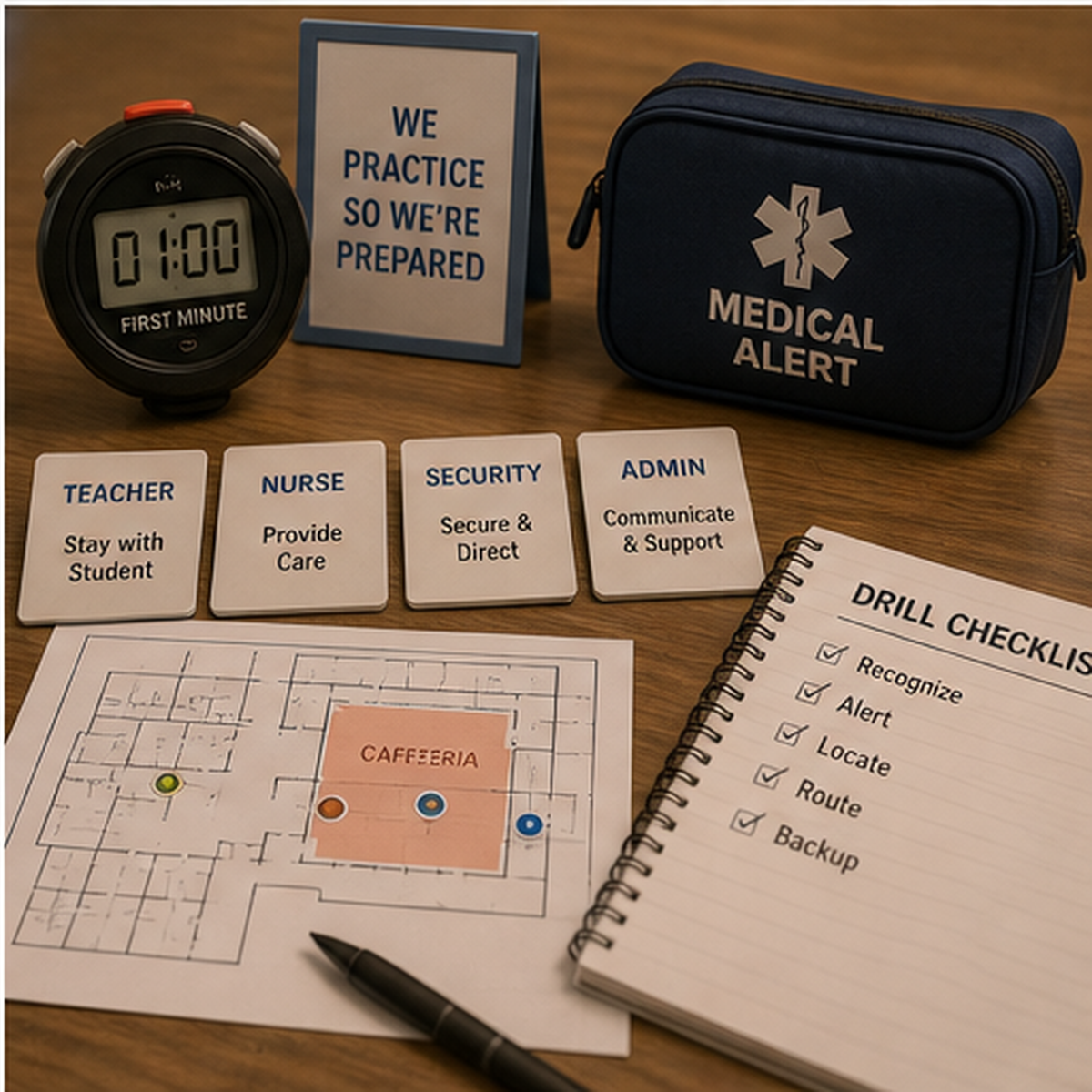
What matters is whether the school can do five things at once when a choking event starts: recognize the emergency, begin the physical rescue sequence immediately, trigger a silent alert without leaving the student, route help to the exact location, and move backup staff and equipment without wasting the next minute in confusion.
The overlap between Alyssa's Law and airway safety is practical. The law pushes schools to modernize the alert layer. Airway emergencies expose whether that alert layer actually supports life-saving response.
If a school still depends on front-office relay, hallway shouting, or somebody running to find help, the system is older than the risk it is trying to manage.
Alyssa's Law infrastructure becomes meaningful when it is tied to drills, location logic, role assignment, and medical escalation planning. The schools that will handle choking emergencies better are not the ones with the loudest alarms. They are the ones that remove delay from the first minute.
It requires schools to have silent panic alert capability that can notify law enforcement or emergency response channels quickly. In states such as New Jersey and Texas, the implementation language makes speed, silence, and direct connectivity core design requirements.
It shortens the time between recognition and coordinated response. The responder can stay with the student while the system pushes location-aware alerts to the people who need to move.
No. Current first-line response for severe choking still depends on trained manual action. The system around the responder exists to reduce communication delay, not replace the rescue sequence.
As a second-line backup only. FDA's QXN category defines suction anti-choking devices as second-line treatment after unsuccessful use of a basic life support choking protocol.
New Jersey Alyssa's Law (P.L.2019, c.33) - Supports New Jersey requires public elementary and secondary school buildings to be equipped with panic alarms directly linked to law enforcement.
Texas S.B. 838 (Alyssa's Law) - Supports Texas requires each classroom to have silent panic alert technology and includes location with alerts.
AHA 2025 Child FBAO Algorithm - Supports Current child severe choking sequence is repeated cycles of 5 back blows followed by 5 abdominal thrusts.
FDA Safety Communication, March 4, 2026 - Supports Established choking rescue protocols should come first; anti-choking devices should only be considered after unsuccessful standard measures.
FDA De Novo DEN250012 / QXN - Supports QXN established as Class II suction anti-choking device as a second-line treatment after unsuccessful BLS choking protocol.
American Red Cross Adult & Child Choking First Aid - Supports Red Cross public first-aid guidance also uses 5 back blows followed by 5 abdominal thrusts for adults and children.
This article is for educational and preparedness purposes only. It is not medical advice, diagnosis, or treatment. In a choking emergency, call 911 or your local emergency number immediately and follow current accredited first-aid guidance. Any suction anti-choking device should only be considered after standard choking rescue measures are unsuccessful, consistent with current FDA public guidance.




















