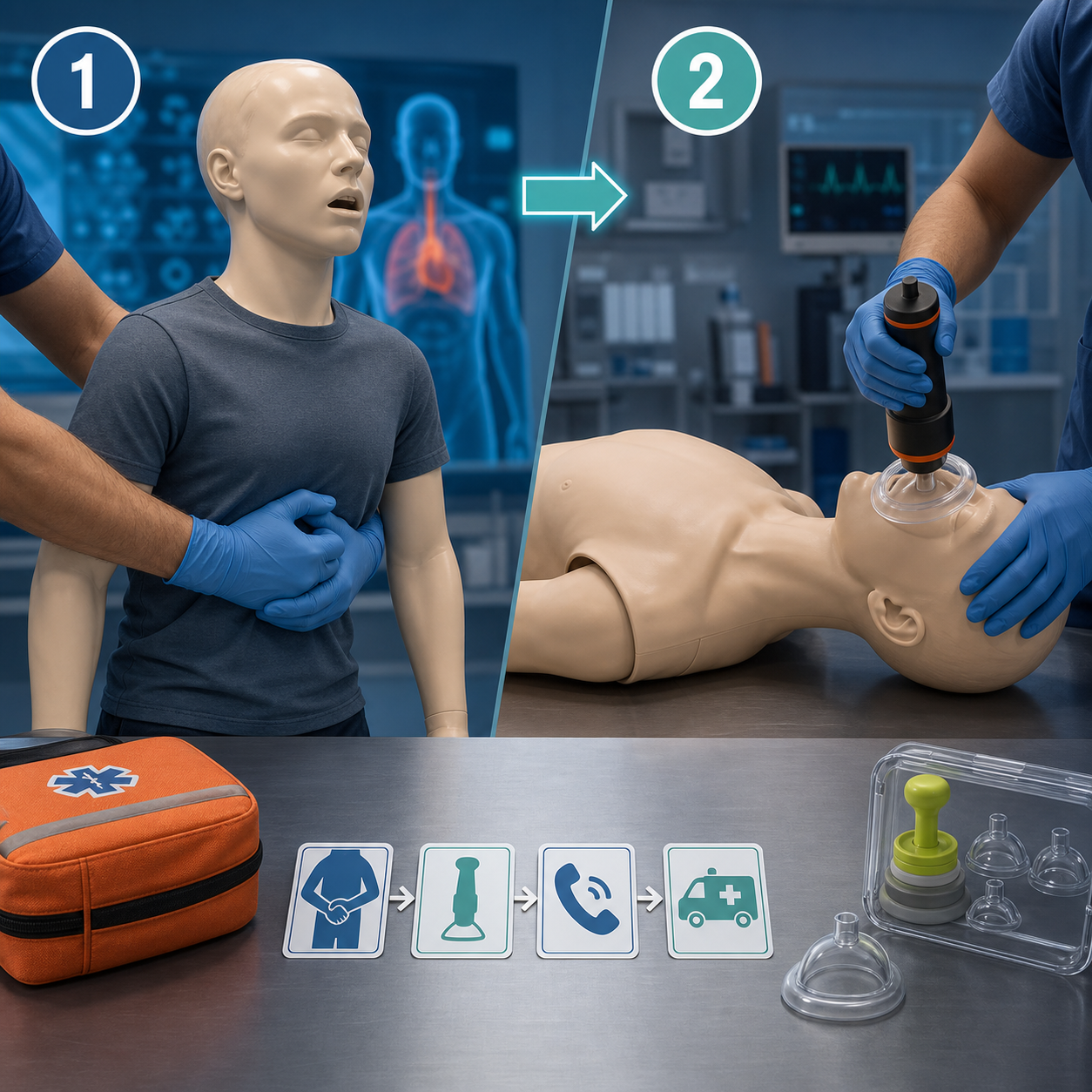
Manual choking rescue still comes first. Under the 2026 FDA framework, a QXN suction anti-choking device under 21 CFR 874.5400 is a second-line option after unsuccessful basic life support choking protocol. The comparison is sequence, not rivalry: 2025 AHA guidance starts with 5 back blows alternating with 5 abdominal thrusts for conscious children and adults.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
The question sounds simple because families, schools, restaurants, and care teams want a clean winner. A choking emergency does not reward that framing. The useful question is: what should happen first, what should happen if it fails, and what mechanical pathway is being used at each step
The old comparison - anti-choking device versus Heimlich - hides the real operating sequence. First-line manual rescue tries to expel the obstruction by creating force from inside the body. A suction anti-choking device creates negative pressure from outside the airway opening. The two methods do not occupy the same position in the 2026 rescue chain.
For a conscious child or adult with severe choking, the 2025 AHA update moved away from a single-technique message. The current sequence is repeated cycles of 5 back blows followed by 5 abdominal thrusts until the object comes out or the person becomes unresponsive. For infants, the sequence is different: 5 back blows followed by 5 chest thrusts. Infant abdominal thrusts are not the recommended first-line action because of injury risk.
The FDA framework created on March 4, 2026 does not replace that sequence. It defines a regulated device category for suction anti-choking devices as a second-line treatment after unsuccessful use of a BLS choking protocol. The practical translation is blunt: recognize severe choking, call 911 or delegate the call, start the age-correct first-line sequence, and use a properly labeled FDA-authorized QXN device only within its intended second-line role.
That order protects time. A device stored across the room cannot beat a rescuer whose hands are already on the victim. A device can still matter after manual rescue fails, when the obstruction is not moving, the rescuer cannot generate effective force, or the victim's body position makes abdominal thrusts less effective.
Manual choking rescue has three advantages that no device can erase: immediacy, availability, and low setup burden. A trained rescuer can begin back blows within seconds. Abdominal thrusts require no cabinet, no packaging, no mask selection, and no device orientation. In a hypoxia event, setup delay is not a small inconvenience. It is biology turning against the victim.
Manual rescue also works through the victim's own pressure system. Back blows deliver a sharp mechanical impulse to the upper back. Abdominal thrusts compress the upper abdomen upward and inward, raising pressure inside the thorax and airway in an attempt to expel the obstruction. The mechanism is positive pressure from inside the body.
The weakness is not the concept. The weakness is execution under real conditions. Frail bodies, obesity, pregnancy, wheelchairs, narrow spaces, panic, poor rescuer position, weak thrusts, and delayed recognition can all lower the effective pressure delivered to the obstruction. A school cafeteria, nursing-home dining room, or restaurant booth does not behave like a training manikin.

A suction device introduces a distinct mechanical pathway: outward pressure differential at the airway opening replaces internal thoracic displacement. The device must create a face seal, generate negative pressure, and transfer that pressure to the obstruction without losing too much force through leaks around the mask or mouth.
That pathway can be valuable after first-line rescue fails. It is not automatically superior. It depends on seal quality, victim size, mask fit, operator training, device condition, and whether the product is actually authorized for the population being treated. A suction device with weak pressure, poor labeling, or vague marketplace claims can create delay without adding reliable rescue value.
The correct comparison is not "Which is better " The correct comparison is "Which force path belongs at this moment of the rescue "
Foreign-body airway obstruction is a mechanical failure. Food does not clear because people believe harder. It clears when enough useful force reaches the obstruction in the right direction before oxygen loss becomes irreversible.
Food texture changes the load. A mechanical simulator study of tongue-palate compression found that clearing a starch-based material required about 5.4 kPa, while clearing a gum-based sample required about 1.7 kPa, despite equal apparent viscosity. That figure is not a rescue-device treatment threshold, and it does not prove that a specific choking event needs exactly 5.4 kPa. It does show why solid, sticky, starch-heavy boluses can demand more mechanical work than soft gel-like material.
Negative-pressure performance also varies. A 2025 preliminary comparison of anti-choking devices reported about 154 +/- 57 mmHg, or roughly 20.5 +/- 7.6 kPa, for one device configuration versus about 62 +/- 29 mmHg, or 8.2 +/- 3.9 kPa, for a lower-performing comparison. The number is useful because it shows the engineering spread: pressure generation is not a marketing slogan. It is a measurable performance variable that can be diluted by leaks, poor fit, or weak device design.
The strongest second-line argument is not that manual rescue is obsolete. It is that manual rescue can fail for physical reasons. A regulated backup can give the response chain another force path when the first one has not moved the obstruction.
|
Rescue dimension |
First-line manual protocol (AHA 2025) |
Second-line suction device (QXN category) |
|
Regulatory position |
Established choking rescue protocol; starts immediately after severe choking is recognized. |
FDA-authorized category under 21 CFR 874.5400 as second-line treatment after unsuccessful BLS choking protocol. |
|
Physical mechanism |
Back blows plus abdominal thrusts use external strike and positive pressure from thoracic or abdominal displacement. |
Mask seal plus negative pressure creates outward suction at the airway opening. |
|
Sequence for conscious child/adult |
5 back blows alternating with 5 abdominal thrusts until object clears or victim becomes unresponsive. |
Not first-line. Consider only after first-line steps are unsuccessful and within the device labeling and training plan. |
|
Force challenge |
Effective pressure depends on rescuer strength, body access, victim position, and technique quality. |
Pressure depends on device generation, mask fit, seal integrity, victim anatomy, and operator sequence. |
|
Engineering evidence point |
Solid or starch-based boluses may require higher clearing pressure than gel-like material in simulator testing. |
A preliminary comparison reported about 154 +/- 57 mmHg for one device configuration versus about 62 +/- 29 mmHg for a lower-performing comparison. |
|
Main advantage |
Immediate, equipment-free, teachable across homes, schools, restaurants, and care facilities. |
Adds a distinct mechanical pathway after unsuccessful first-line rescue. |
|
Main risk |
Weak, delayed, incorrectly delivered, or physically impossible thrusts may fail. |
Misuse, poor seal, unauthorized products, storage delay, or use before first-line rescue can waste critical time. |

|
Moment in the event |
Correct action |
Why it matters |
|
Mild choking |
If the person can cough forcefully, speak, cry, or move air, stay close and encourage coughing. |
A strong cough is an effective clearing mechanism. Unneeded intervention can worsen the obstruction. |
|
Severe choking recognized |
Call 911 or assign a caller. Start age-correct first-line rescue immediately. |
Activation and intervention must occur together. The phone call does not reopen the airway. |
|
Conscious child or adult |
Use 5 back blows alternating with 5 abdominal thrusts. |
This reflects the 2025 AHA update and keeps the fastest equipment-free response first. |
|
Infant |
Use 5 back blows alternating with 5 chest thrusts. Do not use abdominal thrusts as the infant first-line sequence. |
Infant anatomy changes the safety boundary. They are not smaller adults. |
|
First-line failure or physical limitation |
Use a properly staged, properly labeled FDA-authorized QXN device only as second-line backup when training and policy allow. |
The device adds a different force path after manual rescue has not resolved the obstruction. |
|
Victim becomes unresponsive |
Lower to a firm surface, begin CPR, and follow current training. Check the mouth only for a clearly visible object before breaths. |
The event has moved toward respiratory arrest and cardiac arrest risk. CPR becomes the priority. |
Manual rescue deserves first place because it is fast. First place does not mean guaranteed success. The risk rises when the rescuer cannot position correctly, cannot create enough force, or cannot maintain the sequence under stress. For home readiness planning, compare the EasyPumpVac Home Kit.
These are not arguments against first-line rescue. They are arguments for a response chain that does not stop thinking after the first attempt.
Schools, senior-care facilities, restaurants, and home-safety buyers should stop using loose phrases such as "FDA registered" as if they prove clinical authorization. Registration and listing are not the same as FDA authorization, clearance, or approval. In 2026, procurement files should verify the actual FDA record, regulation number, product code, intended use, contraindications, labeling, and instructions for use. For compact placement and procurement planning, review the FoldPumpVac portable device.

For the QXN category, the essential language is specific: suction anti-choking device as a second-line treatment, 21 CFR 874.5400, after unsuccessful use of a basic life support choking protocol. That phrasing does more than satisfy compliance. It prevents dangerous sequence drift.
A district policy or care-facility SOP should not say "use the device when someone is choking" without context. It should say first-line rescue begins immediately, the second-line device is staged for rapid access, and use follows the device label and local training plan after unsuccessful BLS choking steps. For school deployment planning, review Fitiger Schools.
The honest answer is setting-dependent and sequence-dependent. Manual rescue works better as the first action because it is already present. A suction device may work better as a backup when manual rescue has failed or cannot be performed effectively. The word "better" becomes misleading when it ignores timing.
A useful analogy is not competitor versus competitor. It is primary pathway and redundant pathway. A building with a fire extinguisher still needs evacuation routes. A school with an AED still needs CPR. A choking plan with a second-line device still needs immediate back blows, abdominal thrusts, CPR readiness, 911 activation, and staff who know what severe choking looks like. For broader kit comparison, see Shop All.

Our position is not that a device replaces the Heimlich maneuver or the 2025 AHA sequence. It does not. The correct role for a suction-based choking device is as one component in a layered airway-readiness system: prevention, recognition, first-line manual rescue, 911 activation, second-line backup where authorized and labeled, CPR readiness, and post-incident review. For care-area backup planning, review the EasyPumpVac Airway Clearance Home Kit.
The product layer matters only if the system around it works. A device that is locked away, untrained, poorly documented, or used before established protocols can create a false sense of safety. A device staged in the right place, taught in the right sequence, and bounded by the right regulatory language can reduce delay after first-line failure. For portable staging decisions, compare the FoldPumpVac series.

Anti-choking device versus Heimlich is the wrong mental model. The safer model is sequence. Manual rescue starts because it is immediate. A QXN suction device belongs only as a defined second-line backup after unsuccessful first-line BLS choking protocol, within labeling, training, and policy boundaries.
In the room where someone stops moving air, the order matters. First-line action protects the first seconds. Second-line readiness protects the moment when those first actions are not enough. For household kit planning, compare the FoldPumpVac Home Kit.
No. In the 2026 FDA framework, a QXN suction anti-choking device is a second-line option after unsuccessful BLS choking protocol. For conscious children and adults, current first-line rescue starts with 5 back blows alternating with 5 abdominal thrusts. Call 911 and follow current training.
It changed the sequence language for conscious children and adults. The updated guidance recommends repeated cycles of 5 back blows followed by 5 abdominal thrusts until the object is expelled or the person becomes unresponsive. Abdominal thrusts remain part of the sequence, but they are not described as the only first action.
No. Negative pressure is one performance variable. A device also depends on mask seal, operator training, intended-use population, storage, labeling, and correct second-line timing. Strong suction used too late, on the wrong person, or before first-line rescue can still fail the response chain.
It identifies the FDA regulation for a suction anti-choking device as a second-line treatment. Procurement teams should verify product code QXN, FDA authorization, labeling, IFU, contraindications, and training materials before treating a product as part of an emergency-readiness program.
No. Device placement cannot replace first-aid training, CPR readiness, 911 activation, or age-correct choking rescue. It should be treated as a backup layer after first-line rescue fails, not as a shortcut around established protocols.
FDA Safety Communication - Supports the March 4, 2026 FDA safety communication, first-line protocol language, and FDA-authorized device status. Full link
FDA De Novo Database - Supports decision date, device classification name, regulation number 874.5400, and product code QXN. Full link
FDA De Novo Decision Summary - Supports the wording "suction anti-choking device as a second-line treatment" after unsuccessful BLS choking protocol. Full link
American Heart Association Newsroom - Supports 5 back blows plus 5 abdominal thrusts for conscious children/adults and 5 back blows plus 5 chest thrusts for infants. Full link
HealthyChildren.org / AAP - Supports pediatric FBAO sequence and infant-specific caution. Full link
American Red Cross - Supports public first-aid sequence and CPR transition if the person becomes unresponsive. Full link
Redfearn et al. - Supports 5.4 kPa versus 1.7 kPa clearing pressure for starch-based versus gum-based bolus samples. Full link
Fijacko et al. - Supports reported negative-pressure differences between anti-choking device configurations. Full link
This article is for emergency preparedness planning and education. It is not medical advice, legal advice, diagnosis, treatment, or a substitute for hands-on CPR and first-aid training from qualified instructors. Follow current AHA, American Red Cross, local EMS, school, workplace, and care-facility protocols. Verify FDA authorization, labeling, contraindications, and intended use before making procurement or deployment decisions.




















