Authored by George King
R&D Manager & Emergency Preparedness Specialist at Fitiger Life LLC.
Medically Reviewed by Michael J. Bullock, DNP, MSN, RN
What matters first
If you are choking while alone, call 911 immediately and begin self-administered abdominal thrusts. You can also press your upper abdomen forcefully against the back of a sturdy chair or another firm, safe edge. A suction anti-choking device is not the first step. Treat it only as a second-line backup after standard self-rescue attempts fail.
Most choking instructions assume that another person is nearby. Someone sees the universal choking sign, calls 911, gives back blows and abdominal thrusts, and continues care until the obstruction clears or the person becomes unresponsive.
For a household checklist, see Fitiger's child and home choking safety readiness plan.
When you are alone, that response chain disappears.
You may be standing at a kitchen counter after taking a bite too quickly. You may be eating lunch at your desk after everyone else has left the office. You may be in a hotel room, a parked vehicle, or a quiet break room. No one is watching your breathing change. No one is reaching for a phone. No one is close enough to recognize that you cannot speak.
Planning for choking alone starts with a simple question: what can you reach and do within seconds, before panic and oxygen loss make every task harder?
Manual rescue still comes first. Backup second.
Not every choking episode is a complete airway obstruction. Acting too aggressively during a partial obstruction can make the situation worse.
A person with a partial blockage may still be able to cough forcefully, speak, or draw some air. Forceful coughing is useful. It shows that air is still moving through the airway and may dislodge the object without additional intervention.
A complete airway obstruction is different. You may be unable to breathe effectively, speak, cry, or cough. You may hear little or no sound. That is the point at which immediate emergency action is required.
|
What is happening? |
What you may notice |
What to do |
|
Air is still moving |
You can cough forcefully, speak, or breathe with some difficulty |
Keep coughing. Call for help if the problem does not clear or worsens. Do not treat forceful coughing as a complete airway obstruction. |
|
Air movement is becoming weak |
Your cough becomes weak, breathing becomes more difficult, or you can no longer speak normally |
Call 911 immediately. Prepare to begin choking rescue actions. |
|
Complete airway obstruction |
You cannot effectively breathe, speak, cry, or cough |
Call 911 immediately and begin self-rescue without delay. |
The decision has to be fast, but it should not be careless. A weak cough and a forceful cough are not the same signal.
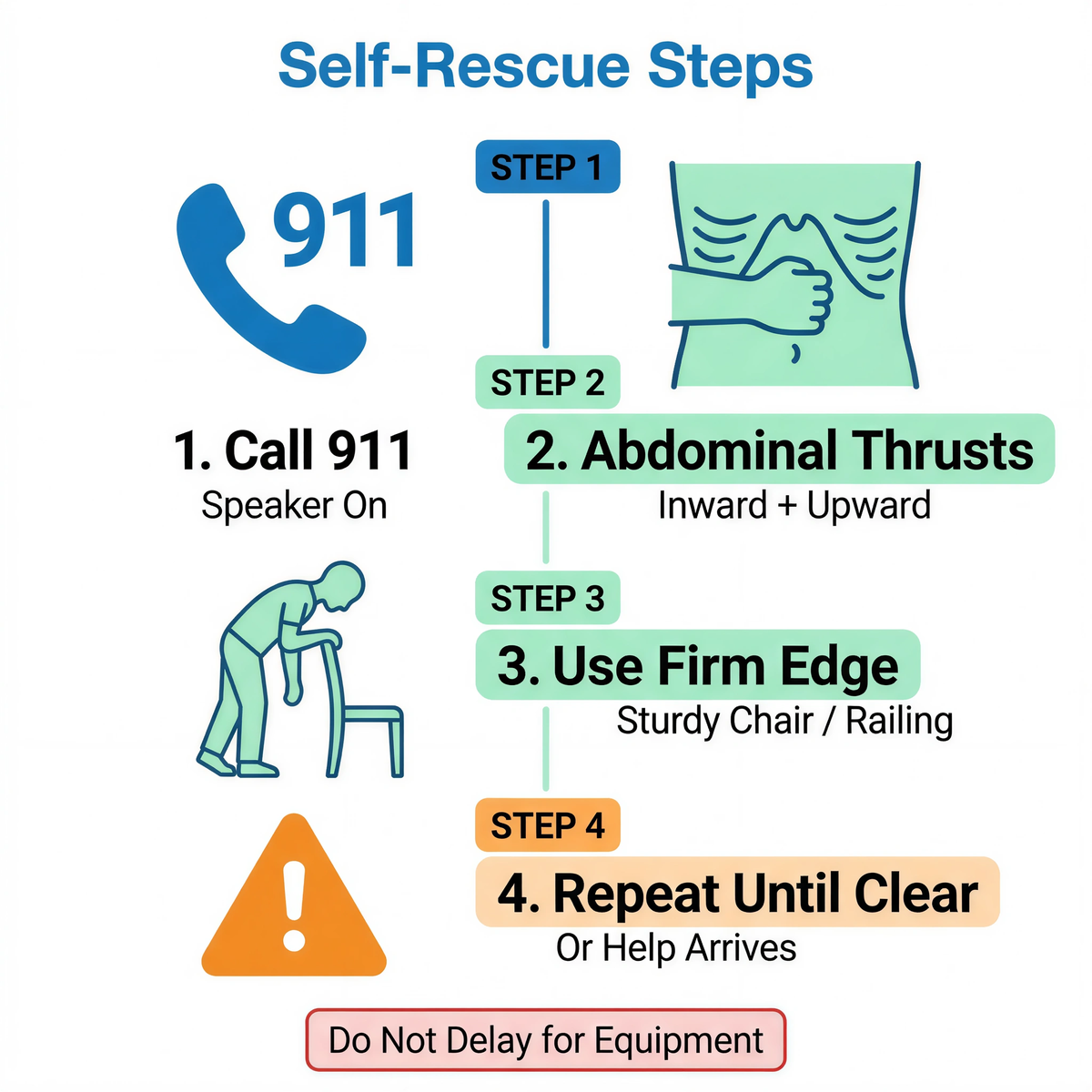
If you have a complete airway obstruction and you are alone, call 911 using a landline or a GPS-enabled mobile phone. Put the call on speaker if possible. Even if you cannot speak, keeping the line open can help emergency dispatchers send assistance.
Begin self-administered abdominal thrusts immediately:
You can also bend over the back of a sturdy chair, a railing, or another firm object and thrust your upper abdomen against the edge. Use a stable surface without sharp corners. A weak folding chair, glass table, unstable stool, or elevated railing can create an additional injury risk.
Do not delay manual self-rescue while opening packaging, assembling equipment, looking for an instruction card, or walking to another room.
A suction anti-choking device is a backup tool. It is not a substitute for self-administered abdominal thrusts, 911, CPR, or first-aid training.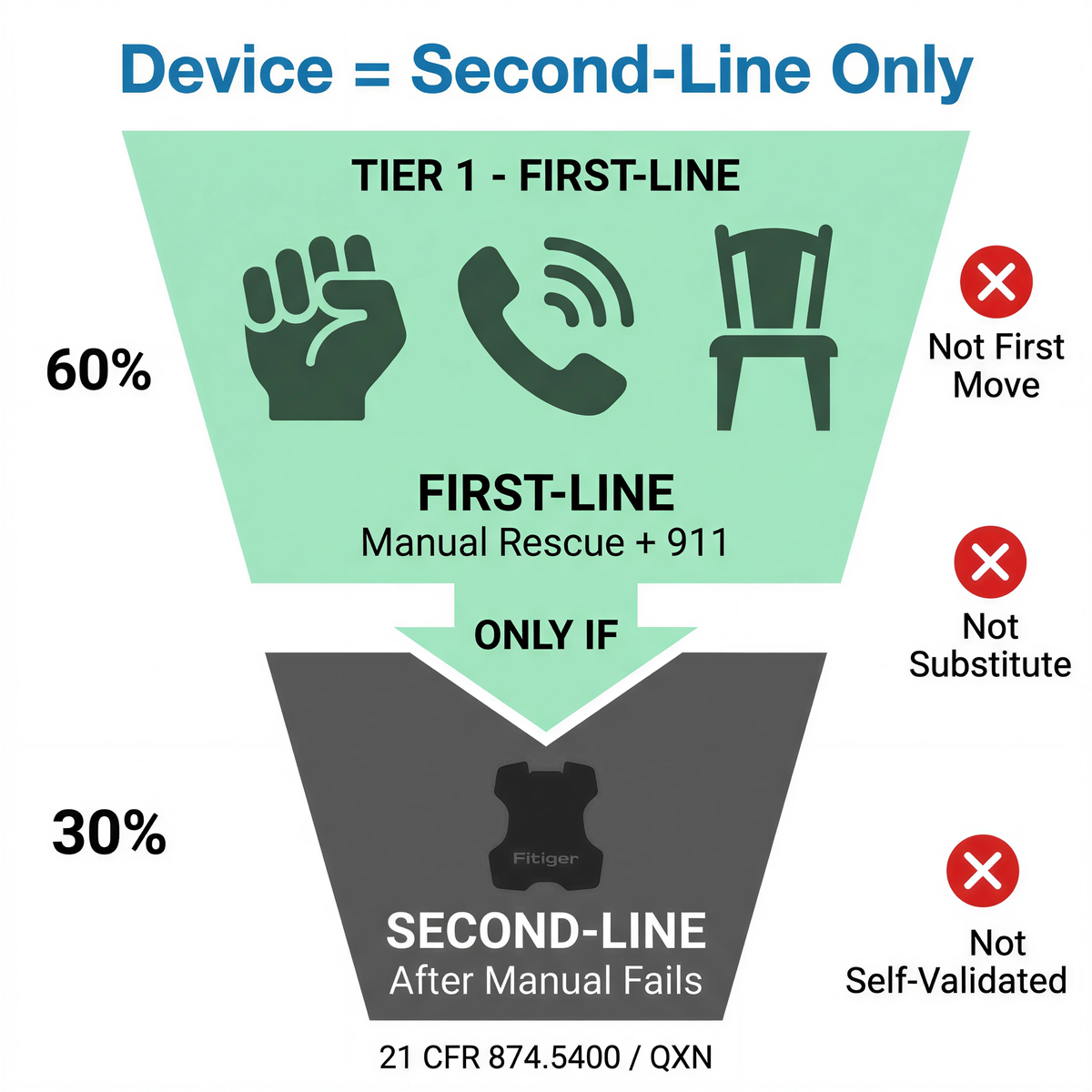
FDA's current framework for this device category is specific. A suction anti-choking device as a second-line treatment is intended for complete airway obstruction after unsuccessful use of a basic life support choking protocol. The category is identified under 21 CFR 874.5400 with product code QXN.
That boundary is especially important when someone is alone.
A choking person may have only a limited window to act. Severe distress can make it harder to open a package, select a mask, position a device, create a seal, and complete the required movement. A device stored in a hallway cabinet may be physically nearby but operationally useless if you are choking at the kitchen table. A backup tool in a vehicle trunk does not help when the driver is seated behind the wheel and cannot get out quickly.
Do not assume that every anti-choking device is authorized, clinically supported, or intended for self-administration. A device sold online may have a familiar shape and confident marketing claims while lacking the labeling, testing, or regulatory status needed for lawful U.S. distribution. FDA registration and device listing do not equal FDA authorization.
Check the current instructions for your specific product before treating it as part of a self-rescue plan. Home use is not the same as self-use. A device may be designed for a trained bystander to use on another person without being validated or labeled for self-administration.
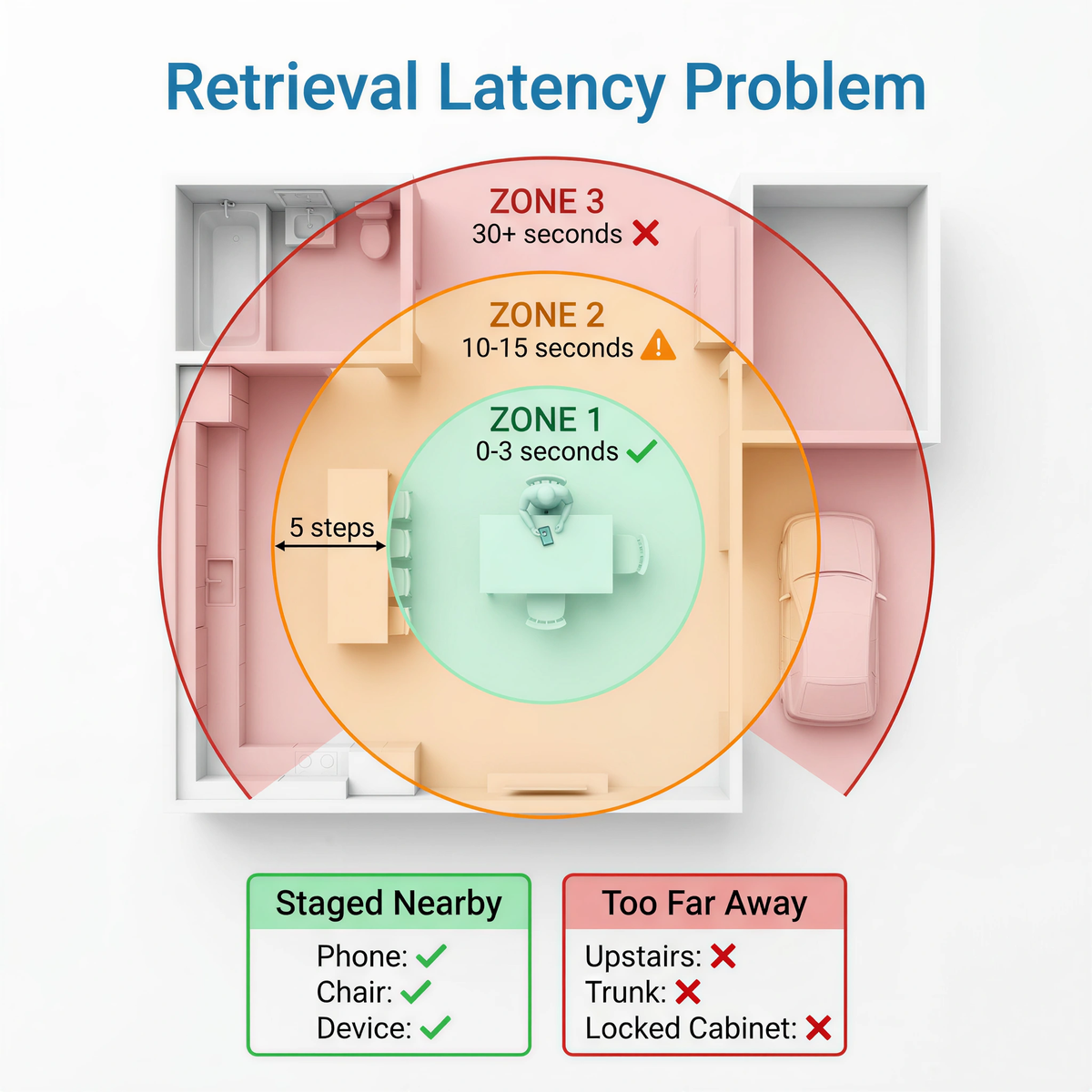
People often focus on whether a device can generate suction. In a real emergency, retrieval latency may decide whether the tool is usable at all.
Retrieval latency is the time between recognizing an emergency and having the correct tool in your hands, ready for use. Every closed drawer, storage pouch, hallway, locked cabinet, unopened box, missing component, or unfamiliar step adds delay.
Consider a person eating alone at home:
The product exists in the home, but the readiness system does not.
A second-line backup should be staged where it can be reached quickly without creating clutter, damage, or accidental access by children. The storage location also needs periodic review. A product that was easy to reach six months ago may be buried behind kitchen supplies after a cabinet was reorganized.
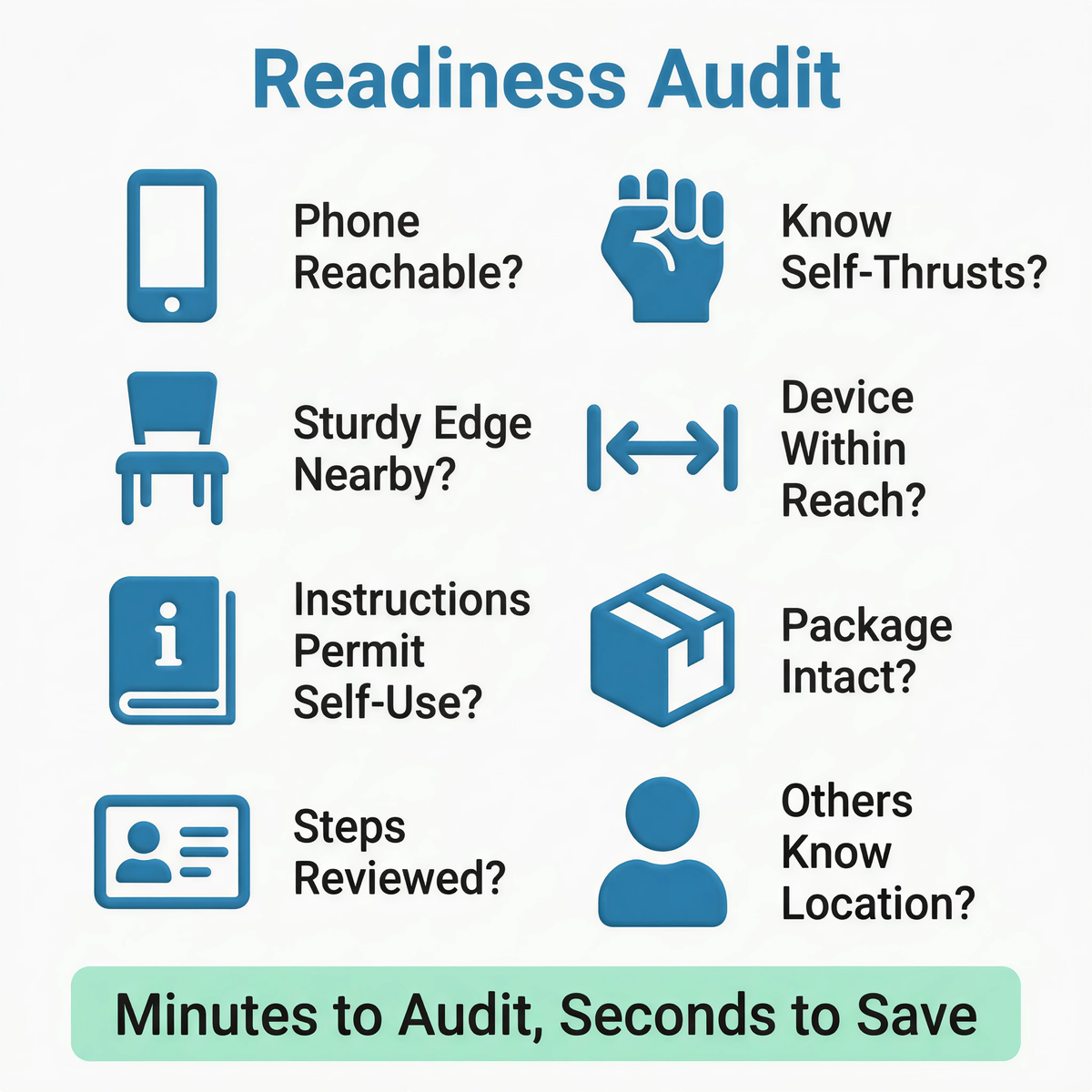
A self-rescue plan should be simple enough to remember under stress.
|
Readiness question |
Why it matters |
What to review |
|
Can you reach your phone from the places where you normally eat? |
Calling 911 early matters when no one else can activate EMS. |
Dining table, kitchen counter, desk, sofa, patio, vehicle, hotel room |
|
Do you know how to perform self-administered abdominal thrusts? |
Manual self-rescue is the immediate first-line action. |
Hands-on first-aid training and periodic review |
|
Is there a sturdy, safe edge nearby? |
A chair back or firm edge may help with self-administered abdominal thrusts. |
Avoid glass, sharp corners, unstable furniture, and elevated railings |
|
Is any second-line device within arm's reach or a few steps away? |
A backup stored too far away may not be retrievable during complete obstruction. |
Kitchen, dining area, workplace desk, vehicle, travel bag |
|
Does the current product instruction permit the use you are planning? |
Home use does not automatically mean self-administration. |
Product-specific instructions for use, labeling, warnings, and training materials |
|
Is the package intact and complete? |
A broken seal, missing mask, damaged part, or opened pouch can disrupt use. |
Monthly visual inspection |
|
Have you reviewed the steps before an emergency? |
An unfamiliar device creates delay at the worst possible time. |
Training card, QR video, practice routine, household review |
|
Does another person know where the device is stored? |
Most emergencies will still involve another rescuer. |
Household members, caregivers, coworkers, restaurant staff |
The audit should take minutes, not hours. The goal is not to turn a home into an emergency department. The goal is to remove avoidable delay.
A suction anti-choking device should not replace immediate manual rescue. Opening a pouch and assembling a device before attempting standard rescue can consume critical time.
A sealed kit in a basement cabinet may be organized. It is not ready. Think about the places where food is actually eaten: the kitchen island, dining table, home office, patio, break room, car, or hotel room.
It does not. FDA authorization is product-specific. Registration, listing, marketplace availability, and advertising language are not substitutes for authorization.
A choking emergency is not the moment to learn how a mask attaches, how a seal is created, or whether the device is intended for the person and scenario in front of you.
Self-rescue has a hard limit. If the obstruction does not clear and you become unresponsive, you cannot continue helping yourself. Early EMS activation is part of the response, not an optional extra step.
A useful plan changes with the environment.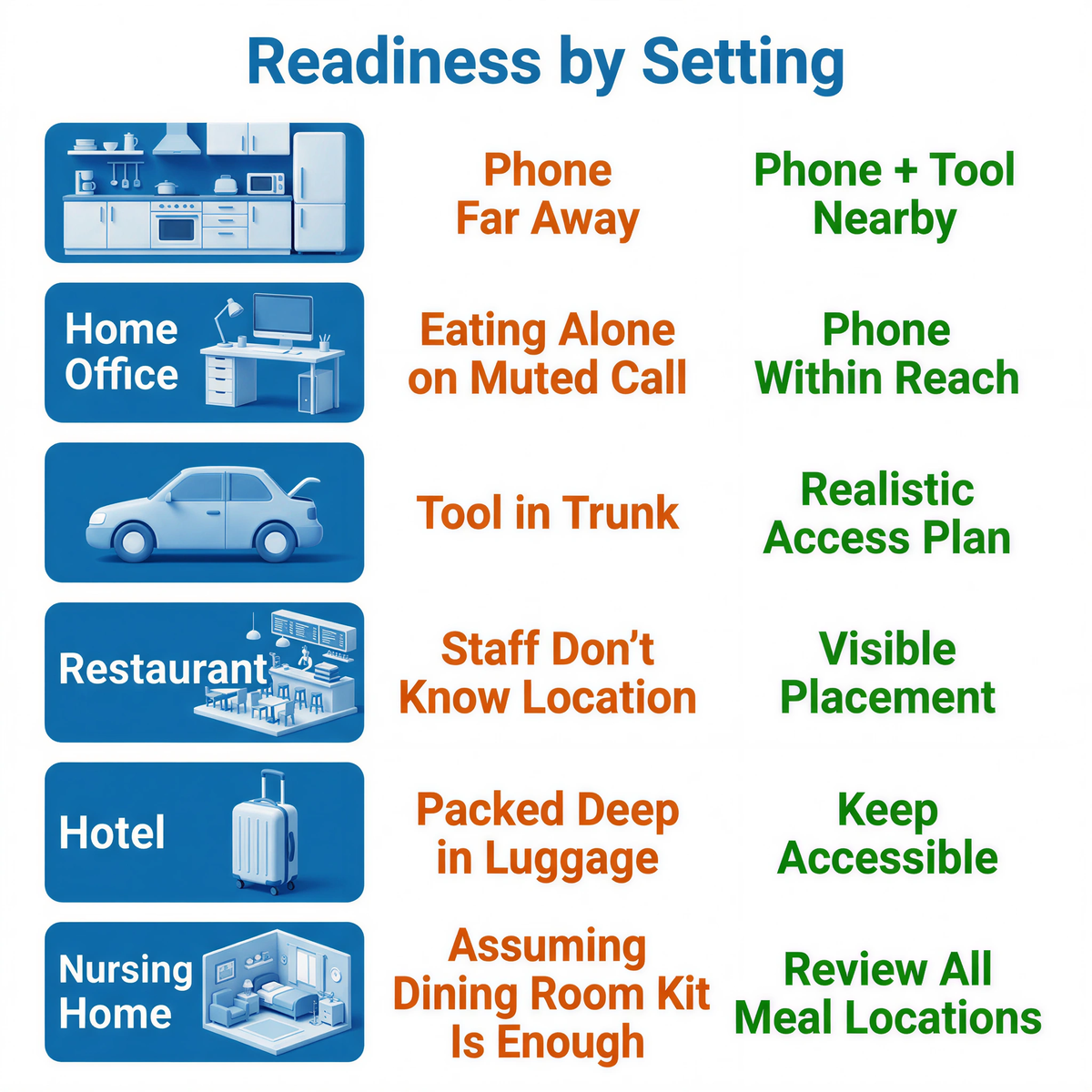
|
Setting |
Common failure point |
Better readiness decision |
|
Home kitchen or dining room |
Phone is charging in another room; backup tool is stored too far away |
Keep a phone accessible during meals and stage any backup tool in a visible, protected location nearby |
|
Home office |
Eating alone during a video call with the microphone muted |
Keep the phone within reach and tell household members where emergency tools are stored |
|
Vehicle |
Tool is stored in the trunk; seat belt and confined space limit movement |
Keep emergency planning realistic. A trunk-only location may create retrieval delay |
|
Restaurant station or break room |
Staff know a device exists but do not know where it is |
Use visible placement, role assignment, and periodic staff review |
|
Hotel or travel setting |
Familiar tools are packed deep inside luggage |
Keep travel readiness items accessible, not buried beneath clothing |
|
Nursing-home resident room |
Staff assume the dining room kit is enough for every location |
Review meal locations, staffing patterns, retrieval routes, and backup placement |
A readiness tool should be placed where people actually live, eat, and move. Storage decisions made for appearance alone often fail during real use.

A self-rescue plan cannot eliminate risk.
A person with complete airway obstruction may panic, lose strength, struggle with hand coordination, or become unresponsive quickly. Some people have mobility limitations, pain, pregnancy-related considerations, or physical conditions that make self-administered abdominal thrusts harder. A first-aid instructor or health professional can help develop a realistic plan for those situations.
A suction device also has practical limits. The mask has to be positioned correctly. A seal has to be formed. The device has to be operated as instructed. The user needs enough physical control to complete those steps while choking.
Treat self-use as an emergency contingency, not as a promise.
A choking incident is not over the instant the object comes out.
Seek medical evaluation after a serious choking episode, especially if abdominal thrusts were performed, a device was used, breathing remains difficult, swallowing feels painful, coughing continues, or the person feels unwell. An object may have caused injury or may not have cleared completely.
Any used emergency device should be handled according to its current instructions for use. Do not casually return a used, opened, damaged, or incomplete product to the cabinet. Inspect the storage location, document what happened, replace components when required, and restage the area.
A readiness system only works when it is restored after the emergency.
If you are planning for choking risk at home, start with first-line rescue training, arm-reach staging, and clear second-line boundaries. Review where you normally eat, how quickly you can reach your phone, and whether any backup tool can be retrieved without delay.
Manual rescue first. Backup second.
For related planning context, review the child and home choking safety readiness plan.
Can I use an anti-choking device on myself if I live alone?
Do not make an anti-choking device your first move. Call 911 and begin self-administered abdominal thrusts immediately. A suction anti-choking device belongs only in a second-line backup role after standard choking rescue attempts fail. Check the current instructions for your specific product before assuming it is intended for self-administration.
What should I do first if I start choking while alone?
Call 911 using a landline or GPS-enabled mobile phone, then begin self-administered abdominal thrusts. You can also press your upper abdomen forcefully against the back of a sturdy chair or another firm, safe edge.
Can I use a chair if I am choking alone?
Yes. A sturdy chair back or another firm edge may help you perform abdominal thrusts on yourself. Avoid sharp corners, glass surfaces, unstable furniture, and elevated railings that could cause a fall.
Should I use an anti-choking device if I can still cough?
A forceful cough usually shows that air is still moving. Keep coughing and monitor the situation closely. Do not treat forceful coughing as complete airway obstruction. Emergency intervention is for a complete blockage or a rapidly worsening situation in which you cannot cough effectively, breathe, or speak.
Are all anti-choking devices FDA-authorized?
No. FDA registration, device listing, online marketplace availability, and advertising claims do not equal FDA authorization. Verify the current regulatory status of the specific product rather than assuming every product in the category has the same status.
Does FDA authorization mean a device should be used before abdominal thrusts?
No. FDA's current framework places suction anti-choking devices in a second-line role after an unsuccessful basic life support choking protocol. Manual rescue comes first.
Where should I store an emergency choking device at home?
Choose a protected location close to the places where food is usually eaten. The device should be easy for an adult to retrieve quickly without being damaged, buried behind supplies, or left where children can reach it. Review the location during monthly inspections.
Should I keep an anti-choking device in my car?
A vehicle kit may be useful for travel readiness, but placement matters. A device stored in the trunk may not be retrievable quickly when someone is seated inside the vehicle. Avoid extreme storage conditions unless the product has been evaluated for them.
Can children use an anti-choking device on themselves?
Do not build a child's safety plan around self-administration. Children need adult supervision, age-appropriate choking prevention, trained caregivers, and rapid access to emergency assistance. Follow the current product instructions and applicable age limits.
What should I do after a choking incident clears?
Seek medical evaluation after a serious choking episode, especially if abdominal thrusts or a device were used, or if symptoms continue. Replace or restage any opened, used, incomplete, or damaged emergency product according to its instructions.
FDA Product Classification — QXN
FDA De Novo Database — DEN250012
American Heart Association — Part 7: Adult Basic Life Support
American Red Cross — Adult & Child Choking: Symptoms and First Aid
Mayo Clinic — Choking: First Aid
This article is for educational and preparedness-planning purposes only. It does not replace medical advice, legal advice, certified first-aid or CPR training, EMS activation, calling 911, professional medical care, local emergency procedures, or the current product-specific instructions for use.




















