The Thomas Telford case is a systems-work failure. Once dysphagia is documented, liability spans texture preparation, tray verification, supervision, first-line rescue, and escalation after manual response fails. In 2026, paper compliance cannot offset tray-level execution drift in regulated care.
For a household checklist, see Fitiger's child and home choking safety readiness plan.
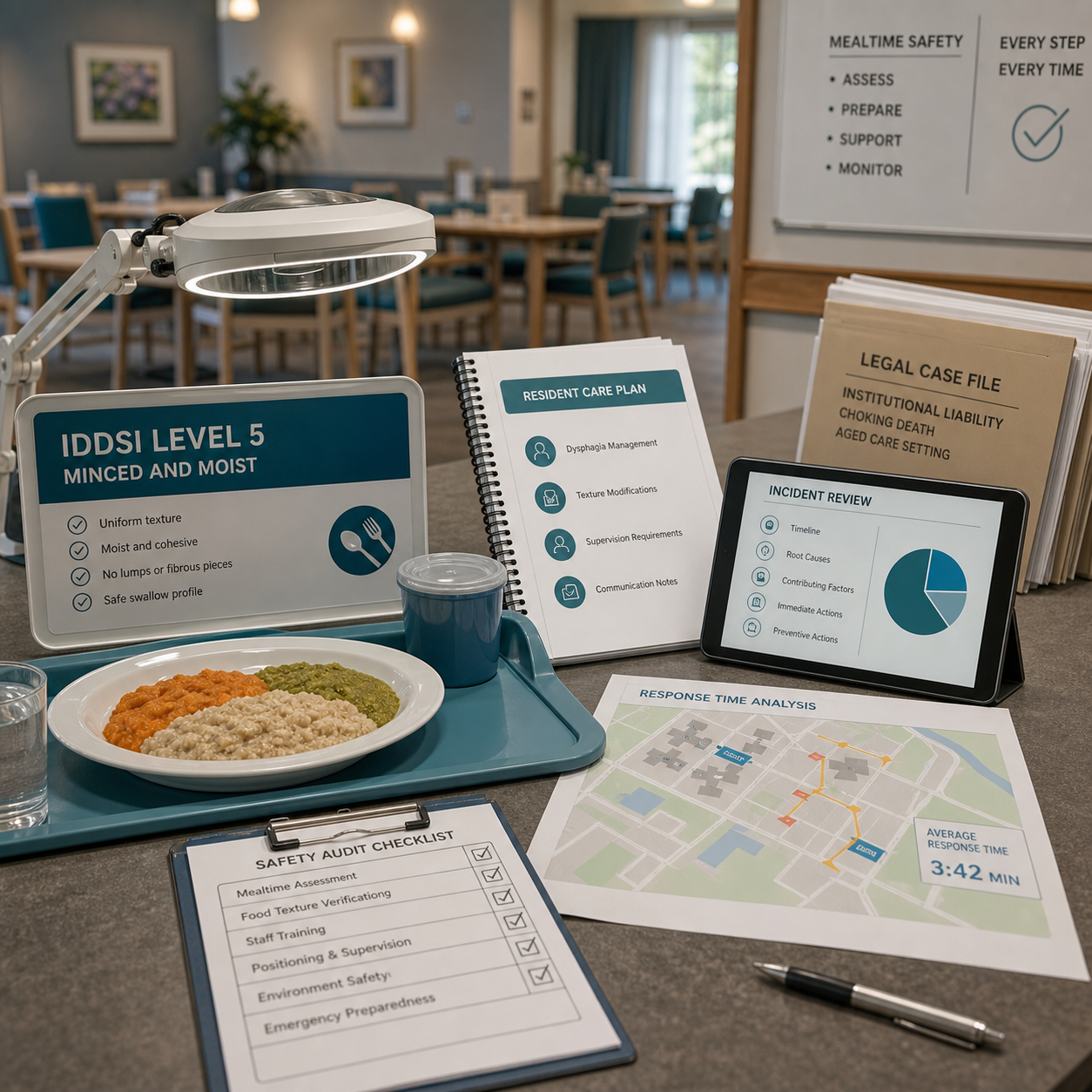
On 6 March 2026, the UK Health and Safety Executive reported that Riverside Care Limited had been fined after Thomas Telford, known as Barry, died following lunch at Riverside Healthcare Centre in Selkirk. HSE said Mr. Telford was 86, had a well-documented history of dysphagia, and had been assessed as needing an IDDSI Level 5 minced and moist diet. The beef served to him had not been prepared to that requirement. Riverside Care Limited pleaded guilty to breaching Section 2(1) of the Health and Safety at Work etc. Act 1974 and was fined GBP 16,000.
This was not framed as an unavoidable collapse. HSE described a failure in the system of work for preparing and serving texture-modified meals. That language moves the case away from one carer, one tray, or one panicked lunch period. The central question becomes whether the provider had built a working chain from swallowing assessment to safe food actually placed in front of the resident.
Food functions as a controlled clinical risk surface in regulated care. A resident with dysphagia is not simply receiving hospitality; the meal is part of the care pathway. The texture, moisture, particle size, supervision level, seating position, and rescue plan all carry operational meaning once the swallowing risk is known.

The visible failure was beef on a tray. The deeper failure was translation. A clinical risk had to pass from assessment, to records, to kitchen preparation, to tray assembly, to dining-room supervision, to emergency response. One broken link was enough to expose the resident to a known hazard.
|
Control layer |
Core failure mode |
2026 defensibility standard |
|
Translation |
Risk was known but not converted into the physical tray. |
Use real-time assessment-to-tray verification. The texture requirement must be visible, current, and checked before exposure begins. |
|
Biomechanical |
The obstructing bolus may exceed the practical clearing limits of routine manual response. |
Train first-line rescue and define a reachable second-line redundancy pathway where policy and device labeling allow it. |
|
Proximity |
Recognition or rescue is delayed because the responder is too far away, blocked by layout, or watching too many residents. |
Map response radius across dining rooms, bedrooms, corridors, and low-visibility seating. |
|
Governance |
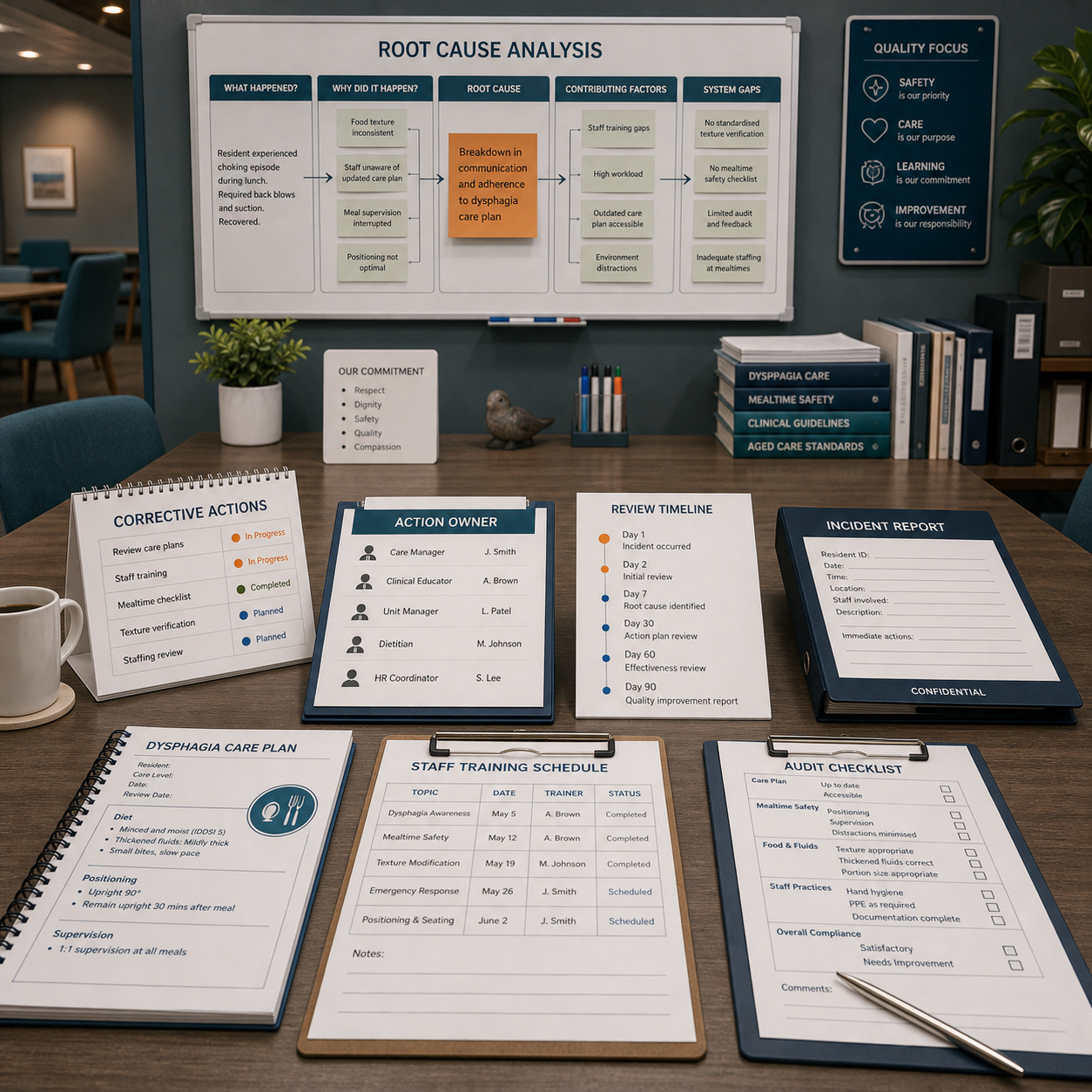
The event is treated as a narrative incident rather than a root-cause failure. |
Every serious choking event or near miss enters RCA/QAPI review with corrective actions and owner names. |
Documentation records a risk. It does not control the tray by itself. Once dysphagia is documented, the provider has to convert the assessment into daily practice: the right food texture, the right supervision, the right staff understanding, and the right escalation path if the resident begins to choke.
CQC guidance on choking risk and dysphagia points care services toward individualized care, current records, IDDSI texture standards, and staff action that reflects swallowing recommendations. A SALT recommendation that sits in a chart but fails to shape the meal is not a working safeguard. Paper compliance fails at the moment the wrong texture reaches the resident.
Manual rescue remains the biological first line. Back blows, abdominal thrusts where appropriate, CPR readiness, emergency activation, and trained staff response cannot be skipped. A credible care-home plan still has to ask a harder engineering question: what happens when those first measures do not clear the obstruction?

Food boluses are not mechanically equal. In Fitiger engineering review work on airway obstruction mechanics, starch-based solid-food boluses can require about 5.4 kPa of release pressure in bench-model analysis, while softer gelatinous materials may require about 1.7 kPa. Those values are not clinical outcome claims. They explain why a dense meat or starch bolus can behave differently from a soft gel and why redundancy planning matters when first-line force transfer fails.
The Thomas Telford case involved beef, a high-risk material for a resident assigned to a minced and moist diet. The key lesson is not that any device should be used first. The lesson is that providers serving known high-risk residents should test the whole pathway, including the seconds after manual rescue fails.
The HSE report said a carer noticed Mr. Telford's lips turning blue and raised the alarm. Blue lips are not an early warning sign. They are a late oxygen sign. A system built around visible crisis has already allowed the resident to move deep into the rescue window.
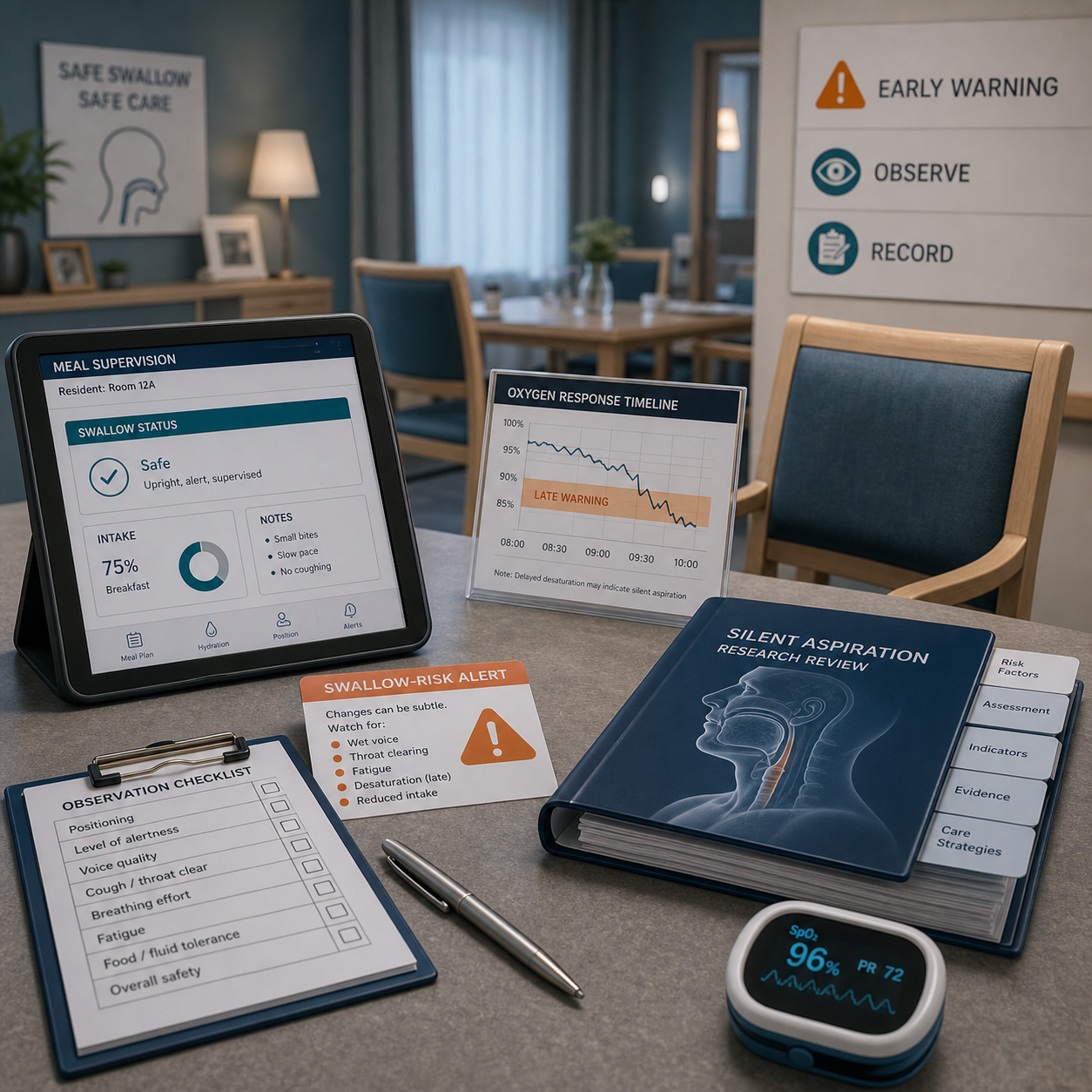
Silent aspiration data adds another warning. In pediatric dysphagia research, oropharyngeal aspiration occurred in 34% of children with feeding difficulties, and 81% of those aspiration events were silent. That population is not the same as an elderly care-home resident, so the statistic should not be transplanted as an aged-care prevalence figure. The systems lesson still holds: airway risk often travels without a loud cough. Neurologic impairment, developmental delay, dementia, stroke history, frailty, and swallowing impairment can all make visible distress an unreliable trigger.
|
Responsibility layer |
What can fail |
Operational control |
|
Assessment |
Dysphagia is recorded but not updated after change in condition. |
Scheduled review, SALT follow-up, care-plan version control, and escalation when coughing, pocketing, fatigue, or recurrent chest infection appears. |
|
Translation |
The care plan uses terms staff or kitchen teams interpret differently. |
IDDSI language, tray cards, visual texture examples, and no informal substitutions such as "soft enough" or "wet bread." |
|
Preparation |
Kitchen output does not match the required level. |
Texture checks, batch separation, allergen/texture labels, and supervisor sign-off for high-risk meals. |
|
Tray verification |
The wrong meal reaches the resident despite a correct plan. |
Final resident-to-tray check before service, not after distress begins. |
|
Supervision |
Known rapid eating, overfilling, fatigue, or poor posture is not controlled. |
Risk-based seating, direct observation, pacing support, and clear stop rules. |
|
Rescue and escalation |
First-line response is attempted but the next action is vague. |
Role assignment, emergency call path, CPR readiness, and policy-approved second-line backup after failed manual protocol. |
|
Governance |
The incident closes as a tragic narrative. |
Root-cause analysis, corrective action, training refresh, evidence of implementation, and board-level review for serious events. |
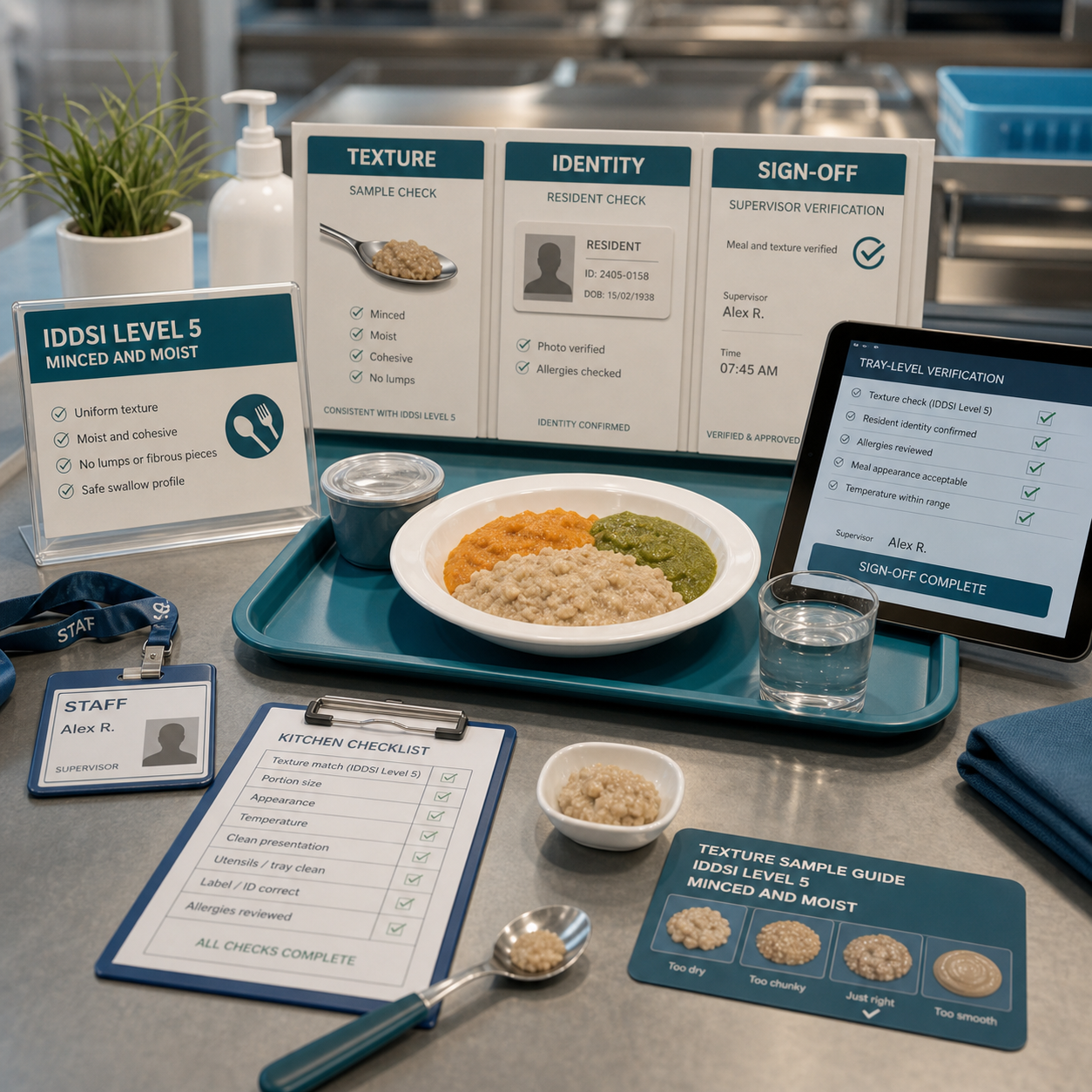
Tray-level verification is the narrow point where paper safety becomes physical safety. A strong system should answer these questions before the resident starts eating:
|
Verification point |
Question to answer |
Evidence to keep |
|
Resident identity |
Is this tray for the correct person? |
Tray card, room/seat confirmation, service check initials. |
|
Texture level |
Does every item match the current IDDSI requirement? |
Kitchen checklist, visual texture reference, batch sign-off. |
|
High-risk components |
Does the tray contain meat, bread, mixed textures, skins, fibrous vegetables, or sticky foods that require extra control? |
Substitution log and supervisor approval. |
|
Supervision level |
Does the person need prompting, pacing, posture support, or one-to-one observation? |
Care-plan field visible to dining-room staff. |
|
Response path |
Can staff call help, begin first-line rescue, and escalate without leaving the resident unsupported? |
Dining-room drill record and equipment reach-time map. |
A second-line device does not repair a failed kitchen process. It does not replace first-line rescue, staff training, CPR readiness, emergency activation, supervision, or medical review. A device also does not erase liability after a known dysphagia risk reaches the tray.
The narrower role is redundancy. FDA's March 4, 2026 safety communication states that established choking rescue protocols come first and that anti-choking devices may be used as a second option if standard protocols are unsuccessful. FDA's De Novo decision for DEN250012 identifies the U.S. device type under 21 CFR 874.5400 and product code QXN as a suction anti-choking device used as a second-line treatment after unsuccessful BLS choking protocol use. That U.S. framework is not a UK care-home mandate. It is useful as a clean engineering boundary: second-line means after first-line failure, not instead of first-line care.
For aged-care providers, the question is not whether a device can make a system safe by itself. It cannot. The question is whether the emergency pathway has a credible next step when manual response fails and the resident is still obstructed.
|
Audit domain |
Failure to look for |
Corrective action |
|
Modified-meal control |
Correct dysphagia note paired with wrong physical meal. |
Build assessment-to-tray verification with named sign-off at kitchen and service points. |
|
Dining-room supervision |
High-risk residents eating quickly, overfilling, or sitting in low-visibility zones. |
Assign seating and supervision by risk, not by convenience or room availability. |
|
First-line response |
Staff know the policy but have not practiced the first 60 seconds. |
Run short choking drills with role assignment, 999/911 activation, CPR readiness, and post-event handoff. |
|
Second-line redundancy |
No realistic plan after manual protocol fails. |
Define whether a policy-authorized QXN-category device is permitted, where it is staged, who may use it, and when it enters the algorithm. |
|
Records and handover |
SALT instructions, meal cards, incident notes, and staff handovers conflict. |
Use one source of truth and audit changes after hospitalization, infection, stroke, decline, medication change, or new coughing episodes. |
|
Governance |
Serious events are written up but not converted into system repairs. |
Route choking incidents and near misses through RCA/QAPI with deadlines, owners, and proof of closure. |
The legal framework changes by jurisdiction. The systems logic does not. Once a provider knows a resident has dysphagia or another swallowing risk, the provider has to control the chain that turns clinical information into the actual dining experience.
In the United States, operators may use different regulatory language: QAPI, risk management, resident safety, facility assessment, staff competency, incident reporting, emergency preparedness, and policy-approved device use. The practical standard is still recognizable. Known risk must be translated into physical controls that work when staff are busy, meals are moving, and a resident cannot protect the airway.
The Thomas Telford case should not be remembered as one unsafe meal. It should be remembered as a failure to hold the full control chain together after dysphagia had already been identified.
A defensible care-home system does not stop at diagnosis. It verifies the tray, supervises the meal, trains the first response, stages escalation, and reviews failures as system evidence. The resident does not choke on paperwork. The resident chokes on the food that reaches the mouth.
The main lesson is that documented dysphagia creates an operational duty. A provider must translate the swallowing assessment into the correct texture, tray verification, supervision, emergency response, and post-incident review. A correct note does not protect a resident if the wrong food reaches the tray.
Dysphagia is a known swallowing risk. Once it is recorded, meal preparation, dining supervision, handover, and emergency response become auditable control points. Liability grows when a provider knows the risk but fails to convert it into reliable daily practice.
No. FDA's 2026 QXN framework describes suction anti-choking devices as second-line devices after unsuccessful BLS choking protocol use. They do not replace prevention, first-line manual rescue, CPR readiness, emergency activation, training, labeling, or medical follow-up.
Tray verification is where care-plan language becomes a physical meal. If the tray does not match the resident's current swallowing requirement, the care plan has failed before the resident takes the first bite.
The provider should audit the full chain: swallowing assessment, IDDSI texture translation, kitchen preparation, tray verification, point-of-eating supervision, first-line response, second-line escalation, incident documentation, and root-cause corrective action.
UK Health and Safety Executive (HSE) - Supports the Thomas Telford case facts, Riverside Care Limited fine, IDDSI Level 5 detail, dysphagia risk, and HSE finding of a failed system of work.
Care Quality Commission (CQC) choking-risk guidance - Supports care-service expectations around choking-risk management, texture-modified foods, thickened liquids, IDDSI adoption, individualized care, and learning from safety incidents.
Care Quality Commission (CQC) dysphagia and thickeners - Supports UK adult social-care guidance on dysphagia, thickeners, and IDDSI-related practice.
FDA Safety Communication, March 4, 2026 - Supports the boundary that established choking rescue protocols come first and anti-choking devices may be used as a second option if standard protocols are unsuccessful.
FDA De Novo DEN250012 decision summary - Supports the U.S. device classification for a suction anti-choking device as a second-line treatment after unsuccessful BLS choking protocol use.
FDA De Novo database entry for DEN250012 - Supports product code QXN, regulation number 874.5400, Class II status, and the De Novo decision date.
Weir et al., Oropharyngeal Aspiration and Silent Aspiration in Children - Supports the statistic that, among children with oropharyngeal aspiration in the study population, 81% had silent aspiration and that silent aspiration was associated with neurologic impairment and developmental delay.
This article is for emergency preparedness planning, product-safety discussion, and educational support. It is not medical advice, legal advice, diagnosis, treatment, or a replacement for hands-on training in CPR, first aid, dysphagia care, SALT guidance, device labeling, local emergency procedures, or professional clinical judgment. Care providers should follow applicable law, regulator guidance, clinical recommendations, device instructions for use, and local emergency instructions. In an emergency, call the appropriate emergency number and follow dispatcher guidance.




















