Manual rescue still comes first. In frail older adults, the event gets harder fast: swallowing risk is already high, the chest is less forgiving, leverage fails more easily in beds and wheelchairs, and once the first maneuver does not clear the obstruction, the next seconds become a force problem, a space problem, and a backup problem at once.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.

|
Mechanical variable |
What changes in aged care |
Why recovery after a failed first attempt gets harder |
|
Thoracic fragility |
Age-related rib and chest-wall changes reduce mechanical forgiveness. |
A maneuver can be both necessary and harder to tolerate when force is concentrated on a brittle chest. |
|
Body-size mismatch |
A lone responder may be smaller than the resident and working from a poor leverage path. |
Effective force transfer drops when height, mass, reach, and stance do not line up. |
|
Bed and wheelchair geometry |
Bed height, side rails, armrests, and one-sided access reshape body position. |
Spatial constraints reduce contact quality and make repeat attempts slower and less controlled. |
|
Single-responder interval |
One person may reach the resident before backup arrives. |
After the first failed maneuver, the room may still be short one set of hands. |
|
Second-line boundary |
FDA places QXN devices after unsuccessful BLS, not before it. |
A credible backup only matters if it shortens delay after first-line failure instead of replacing first-line care. |
Generic first-aid language makes choking rescue sound mechanically tidy. Real aged-care events are not tidy. The resident may have kyphosis, reduced trunk control, contractures, pain, a wheelchair frame blocking access, a bed set too high, or a body size that does not match the responder's leverage. A responder may know exactly what to do and still struggle to produce an effective maneuver on the body and in the space in front of them.
Age-related changes in rib structure and rib-cage geometry are part of that problem. Published work on aging ribs and thoracic posture shows that fracture risk increases with age and that chest geometry changes across adulthood into older age. From our engineering side, this is not a training-only issue. It is a force-transfer issue. The maneuver depends on body position, contact point, leverage path, and available working space. Change those variables enough and the same trained movement no longer produces the same result.
Older adults do not receive manual rescue forces on the same chest assumed in a clean training diagram. The classic trauma literature remains useful here. In elderly patients, each additional rib fracture was associated with a 19% increase in mortality and a 27% increase in pneumonia risk. That does not mean a choking maneuver causing a fracture will produce the same outcomes as blunt trauma in every case. It does mean the aged chest has less forgiveness when force is concentrated on it.
Facilities need to keep two truths in view at the same time. Delay is dangerous. Failed rescue is dangerous. A brittle chest is dangerous too. Aged-care planning gets weaker when teams pretend those risks do not coexist. The hard question is not whether manual rescue should happen. It should. The hard question is where the margin begins to collapse once the first maneuver has already failed.
The boundary here has to stay clean. Manual rescue remains first-line. The Red Cross guidance for conscious choking in adults and children over age 1 uses repeated cycles of 5 back blows and 5 abdominal thrusts. FDA's March 4, 2026 De Novo order created 21 CFR 874.5400 for a 'suction anti-choking device as a second-line treatment' and states that the device is intended for complete airway obstruction after unsuccessful use of a basic life support choking protocol. The device category uses product code QXN.
Mechanically, the pathways differ. Abdominal thrusts aim to create a rapid rise in intrathoracic pressure through the thoracoabdominal system. A physiological study in healthy volunteers measured substantial thoracic pressures during abdominal thrusts. The QXN device category, by contrast, is defined by application of suction at the airway opening after failed BLS. One approach depends on effective pressure transmission through the chest and upper abdomen. The other creates controlled negative pressure proximally at the airway interface. Inference: these are not competing versions of the same force path. They are different mechanical strategies, which is exactly why FDA framed suction as a regulated backup after unsuccessful BLS rather than as a replacement for BLS.
That distinction matters in frail older adults. When the chest is less compliant, the responder is smaller, or the body cannot be positioned well, a second-line option can function as mechanical redundancy after physical intervention fails or becomes impractical in the moment. It is still not a replacement for first-line rescue, EMS, or staff training.
Body-size mismatch is one of the least discussed and most practical problems in nursing-home choking response. A smaller caregiver working alone on a larger resident is not facing an abstract staffing challenge. The responder may not be able to create enough effective displacement of the diaphragm and thorax to move the obstruction, especially if the resident is partly trapped by wheelchair arms, side rails, mattress height, or furniture interference.
The direct choking literature here is limited, and that boundary should stay visible. Ergonomic research on patient handling is not choking-specific, but it still makes one point impossible to ignore: bed height, friction conditions, and transfer geometry materially alter caregiver hand and spinal loads. In one boosting study, slide film reduced peak force demands by about 38% compared with a regular sheet. Other ergonomic studies found that higher or self-selected bed heights changed low-back and hand-force loads during patient handling tasks. Those studies do not tell us exactly how much force is lost in a choking rescue. They do support the operational point that leverage path and setup can materially change what a lone caregiver can do with the same body and the same training.
This topic is not only clinical. It sits inside a 2026 oversight environment. CMS revised Chapter 7 guidance in QSO-26-03-NH and continues to position the Special Focus Facility program as a tool for facilities with persistent poor quality. Separately, the January 2026 Care Compare Five-Star technical guide continues to include 'Percentage of residents experiencing one or more falls with major injury' in the quality-measure domain, while current SFF participants are not assigned star ratings in any domain and instead display a warning sign.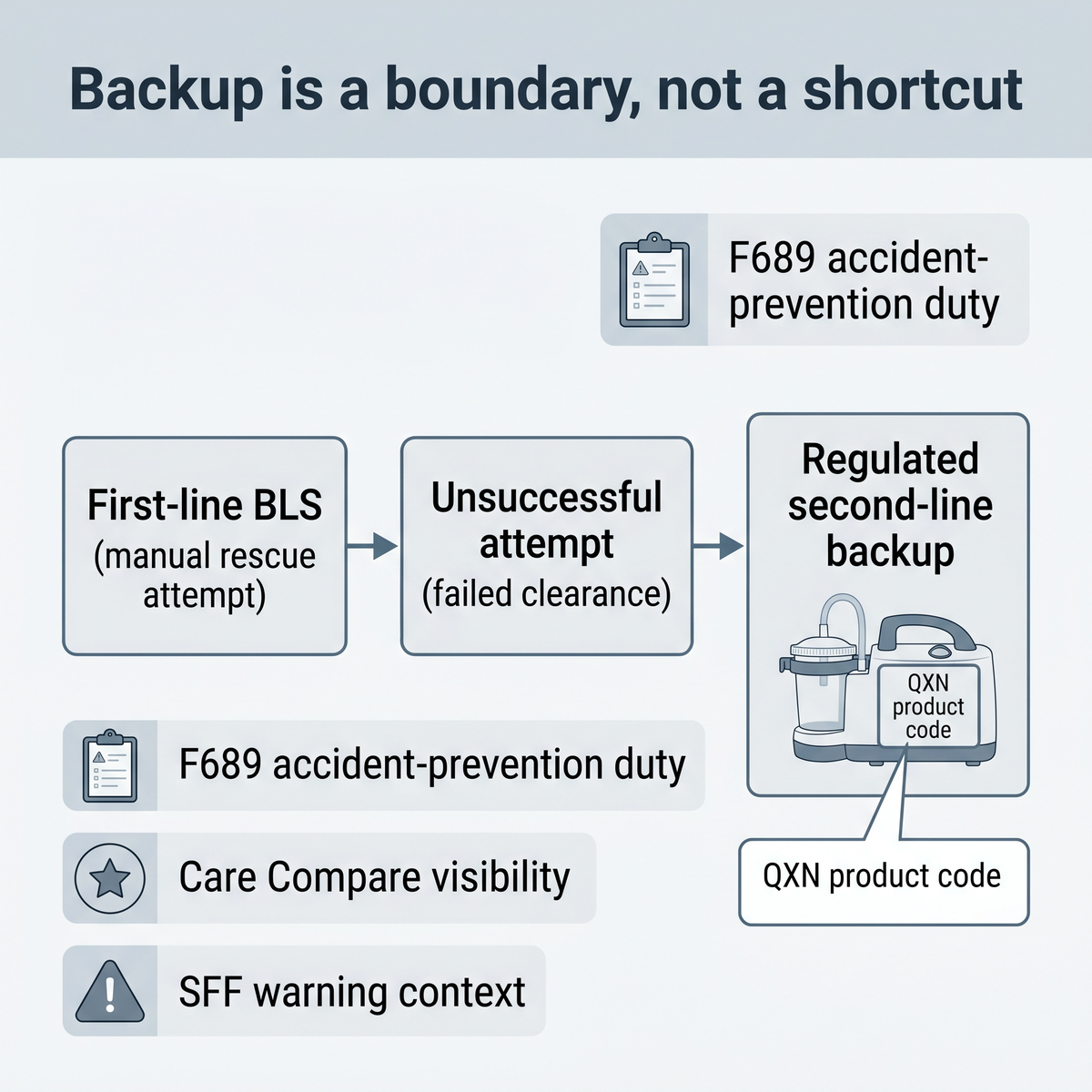
These facts do not turn every rescue injury into a publicly reported quality measure. They do show administrators the environment they are operating in. Major injuries, accident-prevention concerns, and persistent noncompliance do not stay buried inside a single event narrative. F689 still requires adequate supervision and assistance devices to prevent avoidable accidents. A choking response plan that assumes effective manual force transfer in every room, on every body, with every lone responder is an under-planned response model. From a risk-management standpoint, regulated second-line backup is not a marketing detail. It is part of how a facility can reduce exposure after an unsuccessful first maneuver without crossing the first-line boundary set by FDA and established choking protocols.
Start with the bodies and rooms where manual rescue is most likely to lose margin. Which residents have marked kyphosis, severe frailty, osteoporosis, contractures, or large body-size mismatch with the staff most likely to reach them first? Which beds, wheelchairs, or recliners make torso access harder? Which rooms reduce leverage because of one-sided access, bed height, or furniture interference? Which shifts are most likely to leave one person alone in the failed-first-attempt interval?
Then audit the bridge between failed first-line rescue and outside help. The real question is not whether the policy binder says manual rescue comes first. It does. The real question is whether the facility has designed a credible next step after unsuccessful BLS on a frail body in a constrained room. That is the point where preparedness stops being generic and becomes operational.
Manual rescue in frail older adults should not be treated like the same mechanical event shown in a generic training diagram. The body is older. The chest is less forgiving. The responder may be smaller. The room may be tighter. The first attempt may fail. The next seconds matter more than most facilities admit.
First-line response still comes first. That does not change. The real aged-care question is whether the facility understands where manual rescue starts to lose margin and whether it has built a lawful, evidence-aware backup after unsuccessful BLS. That is the difference between a poster-level response plan and a system that is actually prepared for the harder version of the event.Does this article say staff should skip manual rescue?
No. Manual rescue remains first-line response. The article focuses on what happens when first-line BLS is unsuccessful in frail older adults and why facilities need a lawful backup for that interval.
What does 21 CFR 874.5400 change for nursing homes?
It creates an FDA-regulated category for a suction anti-choking device as a second-line treatment. The device is intended for complete airway obstruction after unsuccessful use of a BLS choking protocol. It does not replace BLS, training, or EMS.
Why is rib-fracture risk relevant if choking is the bigger emergency?
Because both risks can coexist in frail older adults. Delay is dangerous, but a brittle chest also has less mechanical forgiveness. Facilities need to plan for that narrower margin instead of pretending every body tolerates force the same way.
Is body-size mismatch a real operational problem?
Yes. A lone responder may know the correct maneuver and still lose effective force transfer because of resident size, poor leverage, wheelchair arms, side rails, bed height, or blocked access.
What should administrators audit first?
Start with residents and rooms where manual rescue is most likely to lose margin: severe frailty, kyphosis, osteoporosis, contractures, large body-size mismatch, wheelchair and bed geometry, one-sided access, and units where a lone responder is most likely to face the event first.
FDA De Novo DEN250012 / 21 CFR 874.5400
FDA Safety Communication, March 4, 2026
American Red Cross adult and child choking guidance
Bulger et al., Rib fractures in the elderly
Aging rib structure and thoracic geometry research
2024 dysphagia prevalence meta-analysis in residential aged care
CMS Five-Star Quality Rating System Technical Users' Guide, January 2026
CMS Appendix PP, F689 Accidents
Ergonomic patient-handling literature on bed height and force demand
Boosting-task force study with slide film
This article is for preparedness, engineering, and risk-management education only. It is not medical advice, legal advice, or a treatment guarantee. In a choking emergency, follow established first-line choking rescue protocols, call 911 or local emergency services, and use any anti-choking device only according to its instructions for use and only after unsuccessful use of a basic life support choking protocol when appropriate.




















