A LifeVac alternative should be judged by sequence, not product popularity. AHA 2025 keeps manual rescue first: 5 back blows plus 5 abdominal thrusts for most adults and children, or chest thrusts when abdominal pressure is not feasible. FDA's 2026 QXN framework places suction only after unsuccessful BLS, inside the first critical oxygen window.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
People usually search for LifeVac alternatives after one concern becomes personal: severe choking can move faster than help can arrive. A parent imagines a dinner table. A school buyer imagines a noisy cafeteria. A care facility thinks about night shift, wheelchair positioning, and residents with swallowing difficulty. Those are real concerns, but a product search can still start in the wrong place.
The safer comparison starts with the rescue chain. Recognition comes first. Age-appropriate manual action comes first. Emergency activation comes first. A suction-based device belongs later, as second-line backup after standard measures are unsuccessful and only within the product's instructions for use.
LifeVac and other product names are used here only for identification and comparison. This article is an independent Fitiger buyer-education guide. It does not claim that one product is clinically superior to another without product-specific, comparable evidence.
The phrase 'anti-choking device' can make the product sound like the whole plan. It is not. In 2026, the sequence is the plan.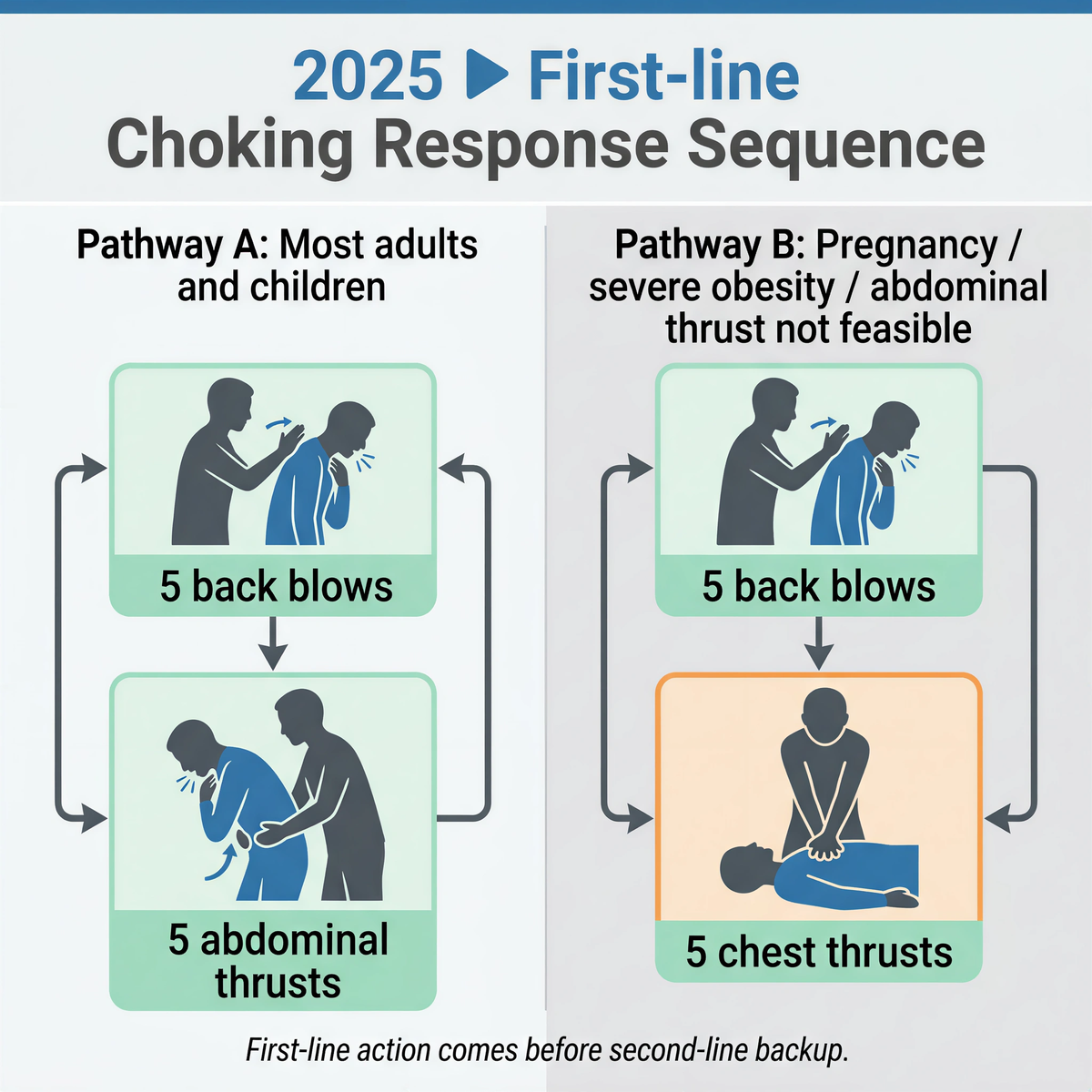
For responsive adults and children with severe foreign-body airway obstruction, the current AHA sequence is repeated cycles of 5 back blows followed by 5 abdominal thrusts until the object is expelled or the person becomes unresponsive. If the rescuer cannot effectively apply abdominal pressure because of pregnancy, severe obesity, abdominal injury, or body geometry, chest thrusts replace abdominal thrusts in the sequence. Infants require a different pathway: back blows and chest thrusts, not abdominal thrusts.
FDA's 2026 public safety language points in the same direction: established choking rescue protocols come first, and suction devices may be used as a second option if standard measures are unsuccessful. The De Novo category under 21 CFR 874.5400, product code QXN, is a second-line category. It is not a device-first category.
Any LifeVac alternative should therefore answer a sequence question before it answers a product question: can the device be staged, retrieved, and understood without delaying the manual protocol that must start first?
A serious alternative is not merely another product with similar packaging or a lower price. It should make the buyer's decision easier across the points that matter under pressure.
|
Buyer question |
What a credible answer should show |
Why it matters |
|
Exact FDA status |
Product-specific status, not vague registration language. |
Prevents buyers from confusing facility registration with device authorization. |
|
Second-line boundary |
Labeling that preserves use after unsuccessful standard choking rescue. |
Reduces device-first delay. |
|
Operation path |
Clear steps, minimal assembly, readable instructions, and realistic hand position. |
Stress makes ambiguous handling worse. |
|
Manual-rescue constraints |
Guidance for pregnancy, severe obesity, wheelchair positioning, or seated posture. |
Some rescue zones change when the rescuer cannot wrap or position effectively. |
|
Seal and mask design |
Mask sizes, seal surface, material, replacement options, and inspection guidance. |
Suction depends on a usable seal. |
|
Evidence boundary |
What testing, reports, and reviews can and cannot prove. |
Protects the buyer from exaggerated claims. |
|
Storage readiness |
Packaging integrity, visibility, replacement parts, and access near likely risk zones. |
A device far from the emergency is operationally absent. |
|
Seller traceability |
Authorized channel, batch, instructions, and support contact. |
Helps reduce copy, old-claim, and unsupported listing risk. |
Marketplace language is often built for speed, not accuracy. A buyer sees 'FDA registered' and may assume the product itself was reviewed for safety and effectiveness. That assumption is not safe.
Registration and listing are administrative concepts. They do not, by themselves, mean a product has FDA approval, clearance, authorization, or a lawful marketing status for the claimed use. In this category, the stronger question is whether the exact product has product-specific support for the intended claim and whether the labeling stays inside the second-line boundary.
LifeVac's 2026 De Novo decision matters because it created a regulated second-line category under 21 CFR 874.5400 with product code QXN. Buyers should not stretch that category into a loose claim for every similar-looking product. A LifeVac alternative should be checked by the same standard: exact product, exact status, exact intended use, exact instructions.
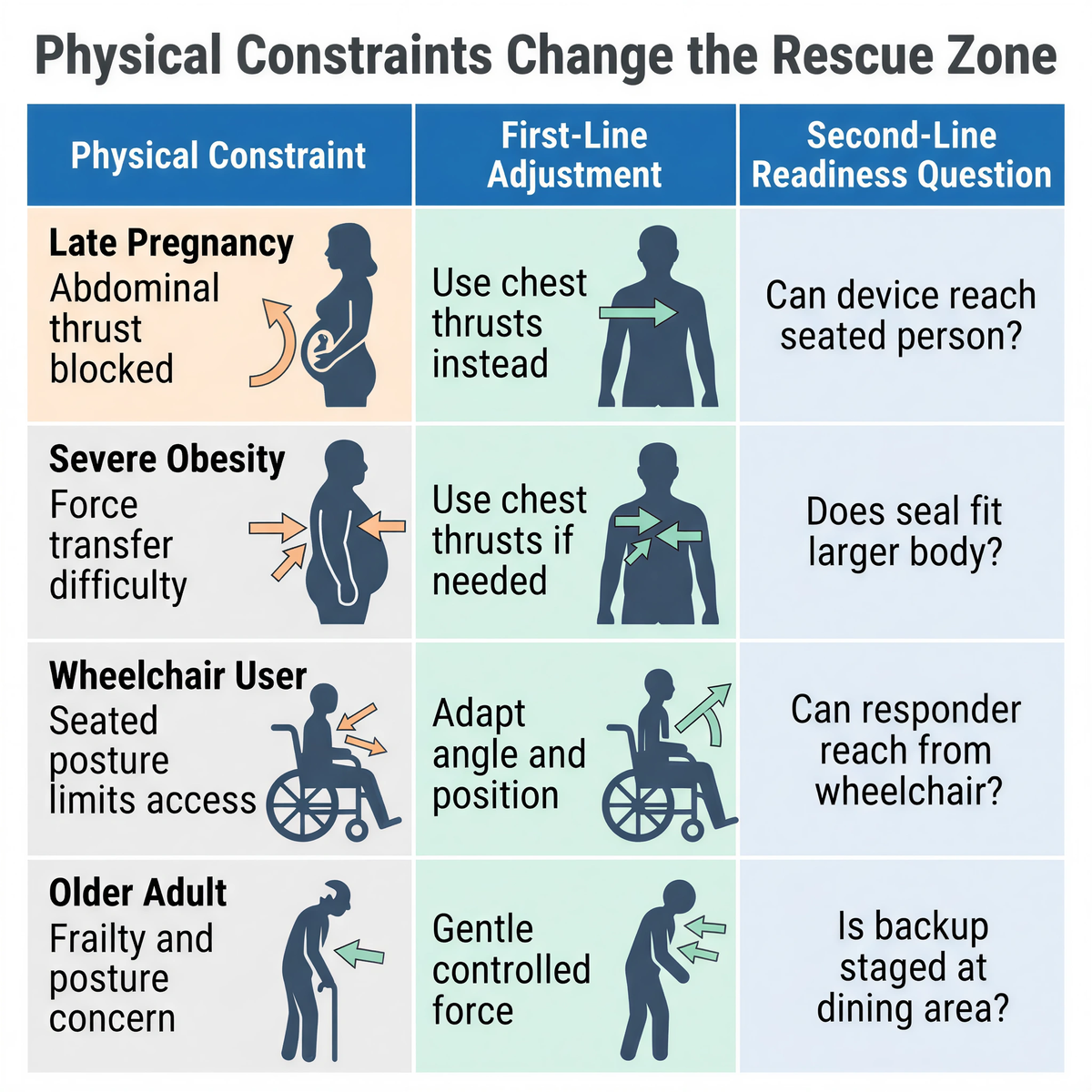
A manual protocol can be correct and still be hard to apply in a real body position. The issue is not whether manual rescue remains first-line. It does. The issue is whether the rescuer can generate the intended force in the intended direction.
Anatomical shifts redefine the rescue zone. In late pregnancy, force moves away from the abdomen and toward the breastbone to protect the uterus while trying to generate intrathoracic pressure. In severe obesity, the rescuer may not be able to wrap the torso or couple force efficiently. In a wheelchair, the backrest, armrests, seated posture, and limited access can block the thrust path or absorb the counterforce.
Food mechanics make that loss of margin easier to understand. Experimental oral-flow simulator work has reported clearing-pressure examples around 5.4 kPa for starch-based material and about 1.7 kPa for gum-based material under tested conditions. Those figures are not clinical thresholds for any product or maneuver. They show a narrower engineering point: bolus material changes the pressure problem. A rescue path that loses force through posture, body geometry, poor coupling, or delayed action has less margin against higher-resistance food behavior.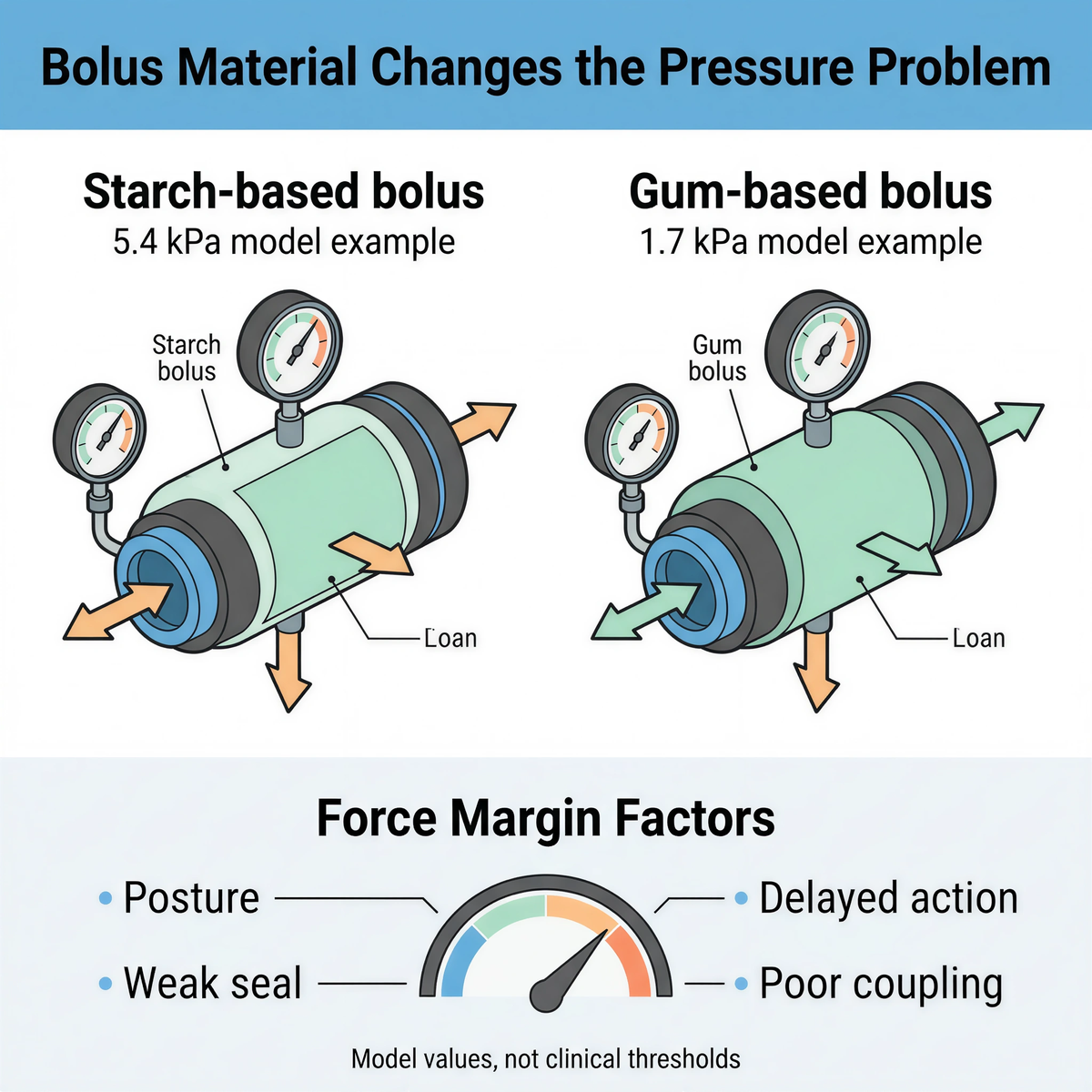
|
Special circumstance |
Physical constraint |
2025 first-line sequence |
Second-line readiness question |
|
Late pregnancy |
Expanded uterus changes the safe force zone and limits abdominal compression. |
5 back blows plus 5 chest thrusts when abdominal thrusts are not feasible. |
Is a second-line QXN-category backup staged without delaying the chest-thrust sequence? |
|
Severe obesity |
Rescuer may not be able to wrap the abdomen or couple force efficiently. |
5 back blows plus 5 chest thrusts when abdominal thrusts cannot be applied effectively. |
Does the response plan reduce retrieval delay after unsuccessful manual measures? |
|
Wheelchair user |
Backrest, armrests, seated posture, and limited space can block or dissipate thrust force. |
5 back blows plus abdominal or chest thrusts as feasible, with positioning adapted to the person and training. |
Is backup staged close enough that the responder does not abandon the person? |
|
Older adult with dysphagia risk |
Reduced swallowing reserve, frailty, dentures, neurologic disease, or seated dependence may raise exposure. |
Same first-line sequence, adapted to posture and responsiveness. |
Does the setting plan account for dining rooms, bedside meals, care carts, and EMS handoff? |

Food choking is often treated as a child-safety topic. That framing misses a major exposure group. Geriatric swallowing literature and public health summaries repeatedly identify older adults as a high-risk population for food choking, and some summaries report that people over 65 have a food-choking incidence about seven times higher than children aged 1 to 4. The exact risk varies by population and dataset, but the planning point is stable: aging, dysphagia, dentition, neurologic disease, reduced cough strength, and seated dependence can turn ordinary meals into higher-risk events.
For a LifeVac alternative search, this changes the buyer question. The product is not being evaluated only for a healthy adult standing in a clear room. It may be evaluated for an older person seated at a dining table, a wheelchair user in a care facility, a resident with dentures, or a caregiver who cannot get behind the person quickly. Access, mask fit, instructions, and staging matter more in those settings than product-page confidence.
A device demonstration happens in clean time. A choking event does not. The rescuer may be untrained, shaken, physically smaller than the choking person, blocked by a chair, or responsible for calling emergency services at the same time.
Compare the operation path without letting product familiarity decide the answer. Count the real steps: choose the mask, attach or verify the mask, position the person, place the device, form a seal, compress if required, pull, reassess, keep emergency services engaged, and hand off to EMS. A design that reduces storage volume or shortens the pull path only matters if it protects this sequence.
FoldPumpVac is relevant to LifeVac-alternative searches because its folding design is built around compact staging. The useful question is not whether folding looks different. The useful question is whether compact storage lets a household, school, vehicle, travel kit, or care setting place second-line backup closer to the likely choking zone.
EasyPumpVac belongs in the same comparison from a different angle: short operation path and compact handling. For buyers comparing device families, that difference should be read as a usability and staging consideration, not as a clinical superiority claim.
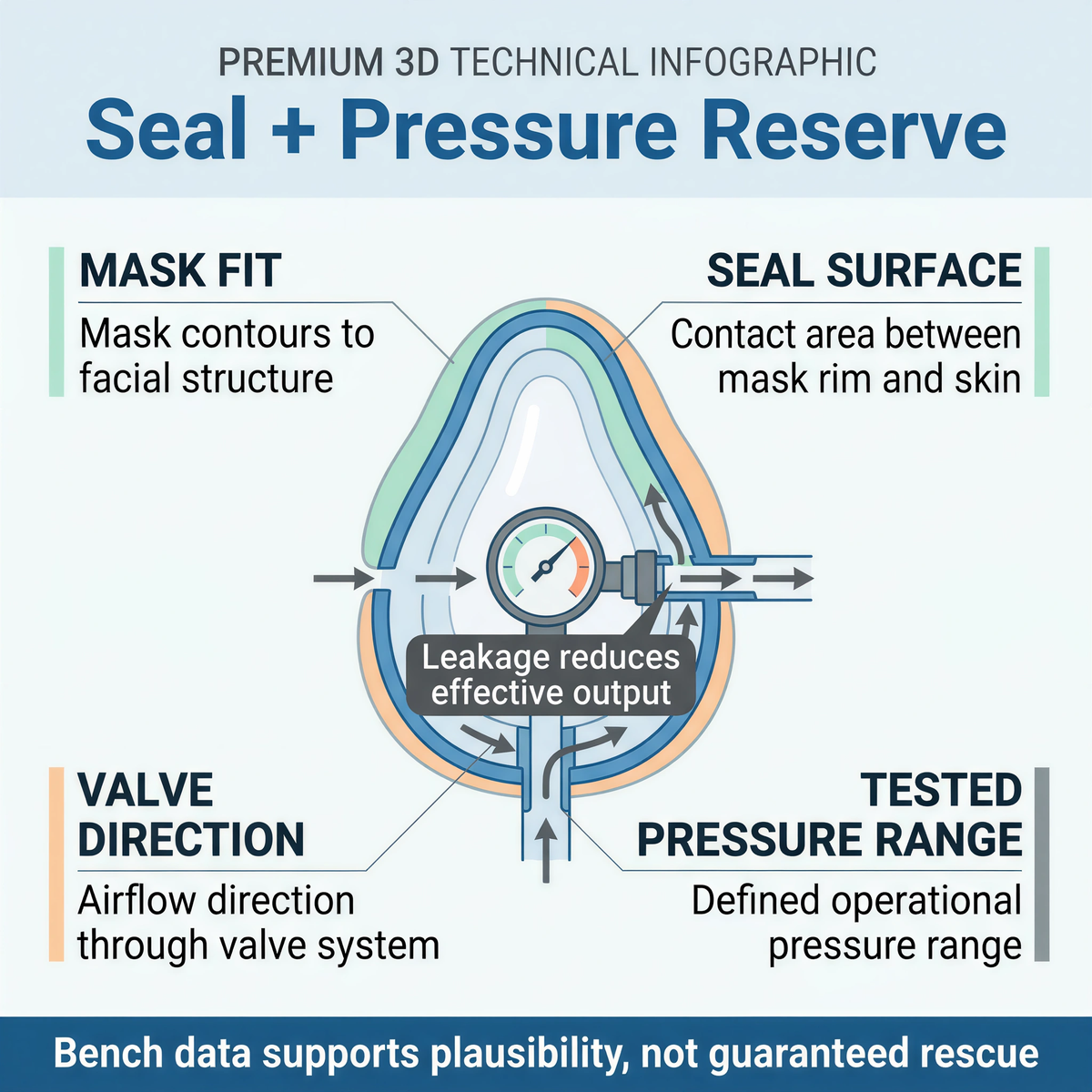
Suction requires a seal. A device body can look solid while effective output collapses through mask leakage, poor facial fit, weak valve control, damaged parts, loose packaging, or unclear replacement options.
Bench data can support mechanical plausibility, but it cannot promise a rescue outcome. Fitiger's evidence materials reference a 19 kPa to 42 kPa pressure/testing range. That range should be read as test-condition evidence, not as a guarantee of clinical success. The useful comparison is more disciplined: what was tested, under what condition, with which device configuration, and what limit does the report not cross?
A low-cost alternative may still look convincing in a product photo. The comparison should move past the photo: mask geometry, silicone quality, valve direction, packaging condition, replacement availability, instructions, storage tolerance, and seller traceability.
Portable design should not be treated as a lifestyle feature. In choking readiness, portability is about retrieval latency.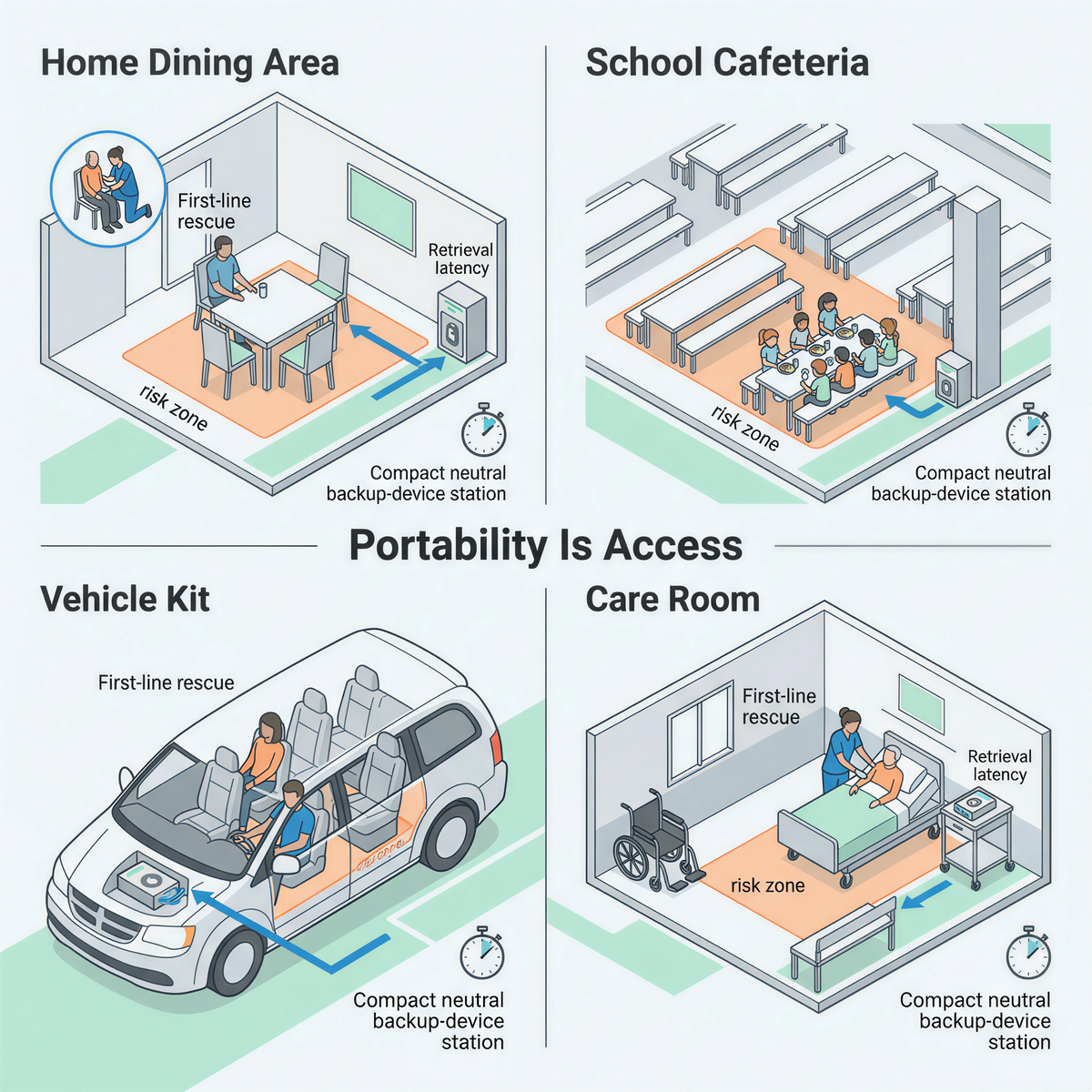
A device stored in a distant cabinet may be legally owned and operationally absent. A device stored in a vehicle but buried under luggage is not staged. A school device locked in a nurse office may be unavailable after dismissal. A care-facility device kept at the central desk may be too far from a private dining room.
FoldPumpVac's folding form should be evaluated against that problem. Compact staging may make it easier to place second-line backup closer to meals, school lunch areas, care carts, vehicle kits, travel bags, and event stations. That does not replace first-line rescue. It reduces one failure mode: distance between the emergency and the backup layer.
Emergency products age inside real environments: closets, cars, gym bags, nurse offices, care carts, dining rooms, school wall stations, and travel kits. Heat, cold, moisture, crushed packaging, opened pouches, missing masks, or separated instructions can weaken readiness.
Fitiger's storage-related materials, including references to extreme-condition evaluation such as low-temperature exposure and boiling-water stress in product-safety discussions, belong in the evidence conversation. They should not be inflated into unlimited durability claims. They show that the brand is asking a practical question: what happens to emergency readiness after storage, transport, and handling?
LifeVac reviews, Dechoker reviews, Fitiger reviews, and Amazon reviews all have a place. They can show packaging experience, instructions clarity, customer support, perceived ease of use, and reported emergency stories. They cannot prove controlled clinical effectiveness.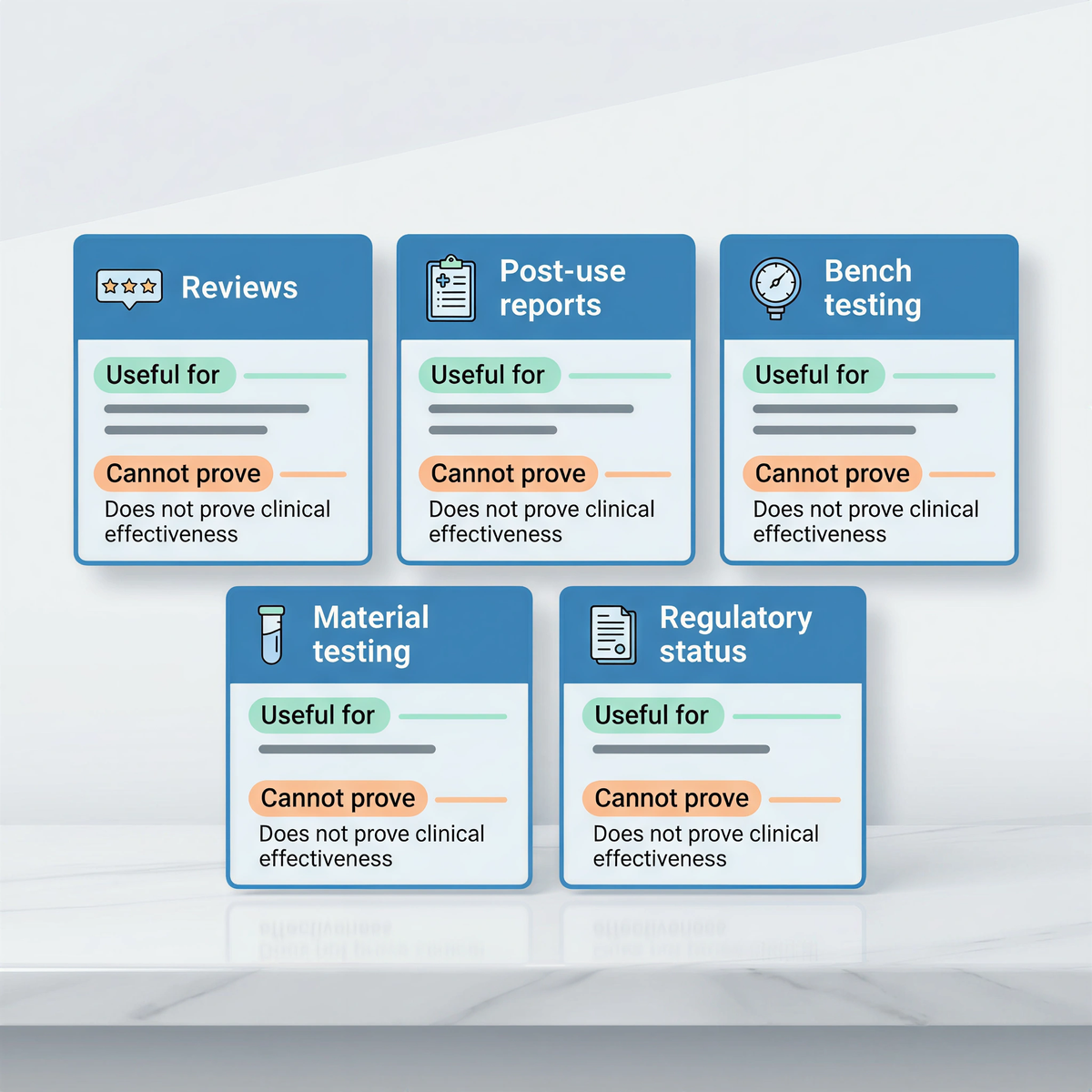
Fitiger has referenced a post-use reporting file of 809 reported emergency airway-clearance uses, with no recorded failed outcome and no recorded oral, facial, or tongue injury report at the time of publication when substantiated. That is a meaningful field-use signal. It is not a randomized clinical trial. It should be read together with bench evidence, material testing, usability evidence, regulatory status, and instructions.
The same rule applies to competitors. A review can be useful without becoming proof. A negative review can identify friction without proving category failure. Evidence discipline protects the reader from both hype and dismissal.
|
Setting |
Buyer priority |
What to compare |
|
Family home |
Dining-area staging, simple role plan, clear instructions. |
Can the device live near meals without being hidden, damaged, or misunderstood? |
|
Cafeteria access, after-school coverage, role assignment, first-line-first policy. |
Can staff retrieve backup without interrupting recognition, 911 activation, and manual action? |
|
|
Older adult risk, dysphagia, wheelchair positioning, night shift, documentation. |
Can staff reach, seal, use, and document the device inside the resident-care workflow? |
|
|
Vehicle or travel kit |
Compact storage, packaging integrity, heat/cold exposure, clear location. |
Can the device remain inspectable and accessible after storage? |
|
Restaurant or event space |
Crowd control, phone access, staff training, EMS route. |
Can the device be staged near dining zones without replacing first-line response training? |
|
Comparison point |
What to check |
Why it matters |
|
FDA language |
Registered, listed, authorized, cleared, or approved - exact wording and exact product. |
Prevents false equivalence between paperwork and product review. |
|
Response sequence |
First-line AHA/Red Cross action first; second-line suction only after unsuccessful standard measures. |
Reduces device-first delay. |
|
Pregnancy/obesity/wheelchair use |
Whether the plan accounts for chest-thrust pathways and positioning constraints. |
Manual force generation changes when abdominal access fails. |
|
Operation path |
Parts, assembly, mask handling, pull path, instructions, reassessment. |
Stress exposes handling friction. |
|
Seal and materials |
Mask fit range, medical-grade silicone, valve control, replacement masks. |
Suction depends on seal quality and contact material. |
|
Pressure evidence |
Test range, setup, limit, and whether the claim applies to the exact device. |
Bench data helps only when scoped correctly. |
|
Portability and staging |
Storage volume, visibility, wall or kit placement, retrieval path. |
Access affects time. |
|
Reviews and reports |
Buyer experience, reported use, follow-up limits, denominator limits. |
Reviews inform; they do not prove clinical superiority. |
|
Seller traceability |
Authorized seller, batch, IFU, support, replacement parts. |
Reduces copy and old-claim risk. |
Fitiger should be evaluated as a second-line backup option inside a broader choking-response plan, not as a shortcut around first-line protocols.
FoldPumpVac fits buyers who care about compact staging, travel readiness, vehicle kits, school kits, and backup access near likely risk zones. EasyPumpVac fits buyers who care about a short operation path, compact handling, and simple staging in a second-line readiness plan. Fitiger's material, pressure, storage, and post-use reporting evidence should be read as product-specific evidence layers, not as universal rescue guarantees.
That boundary is not a weakness. It is what credible airway-safety communication requires in 2026.

Choose the response plan before you choose the device.
Where will the device live? Who may need it? Which first-line protocol applies to that person? What happens if the person is pregnant, severely obese, wheelchair seated, elderly, or physically difficult to reposition? Who calls emergency services? Who retrieves backup? Can the device be reached without leaving the choking person alone?
A strong LifeVac alternative is not the loudest product page. It is the option that fits the sequence, preserves manual first-line rescue, shows credible evidence boundaries, and can be staged where seconds are actually lost.
There is no single best alternative for every buyer. Families, schools, and care facilities should compare FDA language, second-line labeling, operation path, seal design, material evidence, pressure testing, storage readiness, seller traceability, and staging location.
No. Established choking rescue protocols come first. A suction-based anti-choking device belongs only as second-line backup after standard measures are unsuccessful and only within the product instructions.
For responsive adults and children with severe foreign-body airway obstruction, AHA materials use repeated cycles of 5 back blows followed by 5 abdominal thrusts. When abdominal thrusts are not feasible, such as some pregnancy or severe obesity situations, chest thrusts are used instead.
These conditions can change the rescue zone, limit the rescuer’s reach, absorb force, or block body positioning. The manual protocol remains first-line, but the response plan should account for physical constraints before an emergency.
FDA language can mislead buyers when registration, listing, authorization, clearance, and approval are treated as the same thing. Buyers should verify the exact product status and the intended-use boundary.
Pressure evidence helps evaluate mechanical plausibility, seal behavior, and performance reserve under tested conditions. It does not guarantee a rescue outcome and should not be stretched beyond the test setup.
Fitiger should be understood as a second-line backup option inside a broader response plan. FoldPumpVac emphasizes compact staging and portability. EasyPumpVac emphasizes a short operation path and compact handling. Neither replaces first-line rescue, CPR training, 911, EMS, or professional care.
|
Source |
What it supports |
Full link |
|
FDA Safety Communication, March 4, 2026 |
Supports the first-line-first and second-option language for anti-choking devices. |
|
|
FDA De Novo Order DEN250012 |
Supports 21 CFR 874.5400, product code QXN, and second-line suction anti-choking device classification language. |
https://www.accessdata.fda.gov/cdrh_docs/pdf25/DEN250012.pdf |
|
FDA Registration and Listing Reminder |
Supports the distinction that registration and listing do not denote product approval, clearance, or authorization. |
|
|
American Heart Association 2025 Adult FBAO Algorithm |
Supports the repeated 5 back blows plus 5 abdominal thrusts sequence for responsive adults with severe FBAO. |
|
|
American Heart Association 2025 Child FBAO Algorithm |
Supports the repeated 5 back blows plus 5 abdominal thrusts sequence for responsive children with severe FBAO. |
|
|
Food Oral Processing and Tribology review |
Supports the 5.4 kPa versus 1.7 kPa comparison as a model-based food-mechanics example, not a clinical threshold. |
|
|
Age-related swallowing and choking risk literature |
Supports the point that older adults are an important food-choking risk group and should not be treated as an edge case. |
|
|
Fitiger EasyPumpVac Biocompatibility Testing article package |
Supports Fitiger material-contact evidence boundaries for cytotoxicity, irritation, and sensitization summaries. |
|
|
Fitiger product and evidence planning files |
Supports use of FoldPumpVac folding portability, EasyPumpVac short operation path, 19 kPa to 42 kPa testing range, and careful handling of 809 reported post-use file claims. |
https://fitiger.net/blog/detail/fitiger-negative-pressure-testing |
This article is for preparedness, engineering, and buyer-education purposes only. It is not medical, legal, regulatory, or procurement advice. In a choking emergency, follow current first-line rescue protocols, call 911 or local emergency services, and use any suction anti-choking device only as a second-line option after unsuccessful standard measures and only within its instructions for use. Verify the FDA status of any exact product before making claims about authorization, clearance, approval, or classification.
LifeVac and Dechoker are trademarks of their respective owners. Product names are used only for identification and comparison. This article compares publicly available information, response-sequence requirements, design considerations, and evidence boundaries. It does not claim clinical superiority unless directly supported by product-specific, comparable evidence.




















