Workplace choking risk is no longer only a first-aid cabinet issue. In restaurants, hotels, cafeterias, offices, factories, and banquet spaces, OSHA records, incident notes, training files, and public-facing safety data can expose whether the response chain worked or failed. The practical test is reach-time.
For meal-service teams, Fitiger's restaurant choking readiness plan gives practical guidance for staff roles, kit placement, and service-area response.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.

A restaurant can look prepared until a guest at table 14 suddenly cannot speak.
The server sees the face change before the manager does. A tray stand blocks the aisle. The host stand phone is across the room. The first-aid kit is in the office. The manager has the key. The dining room is loud, and the person choking is becoming quiet.
This is the real world behind a restaurant choking emergency plan. It is also why hotels, banquet halls, cafeterias, factory break rooms, office lunch areas, and dense hospitality spaces need more than a generic first-aid statement.
A choking emergency is a floor-design problem as much as a training problem. The room has to answer practical questions under pressure.
A workplace that cannot answer those questions before the emergency is asking its employees to improvise during the emergency.
OSHA does not need a special choking standard before airway emergencies become relevant to workplace safety logic. Employers still have duties around recognized serious hazards. In food-service and dense work environments, choking becomes foreseeable where eating, speed, crowding, distraction, and delayed communication overlap.
That does not mean every choking event becomes an OSHA case. It does mean a site with known bottlenecks should not wait for an incident to discover them.
A banquet room with narrow aisles, a hotel breakfast area with one staff member, a factory break room far from supervisors, or a restaurant floor where only one manager knows where emergency equipment is stored can all carry the same flaw: the response depends on luck.
Restaurants and dense worksites should treat choking readiness as a response-chain audit, not a product-placement afterthought.
Workplace safety events do not always stay inside the building. OSHA posting, electronic injury reporting, establishment search tools, internal incident reports, training records, witness statements, and legal discovery can all make the response sequence visible after a serious event.
A guest choking in a dining room, a worker choking in a break area, or a banquet attendee collapsing during service is not only a medical emergency. It can become a record of what the employer knew, what the plan said, who was trained, where equipment was stored, and how long it took the room to act.
Once the sequence is reconstructed, vague readiness language does not help much.
A backup device in a manager’s office may look like preparedness until the first witness has to leave the person to find it.
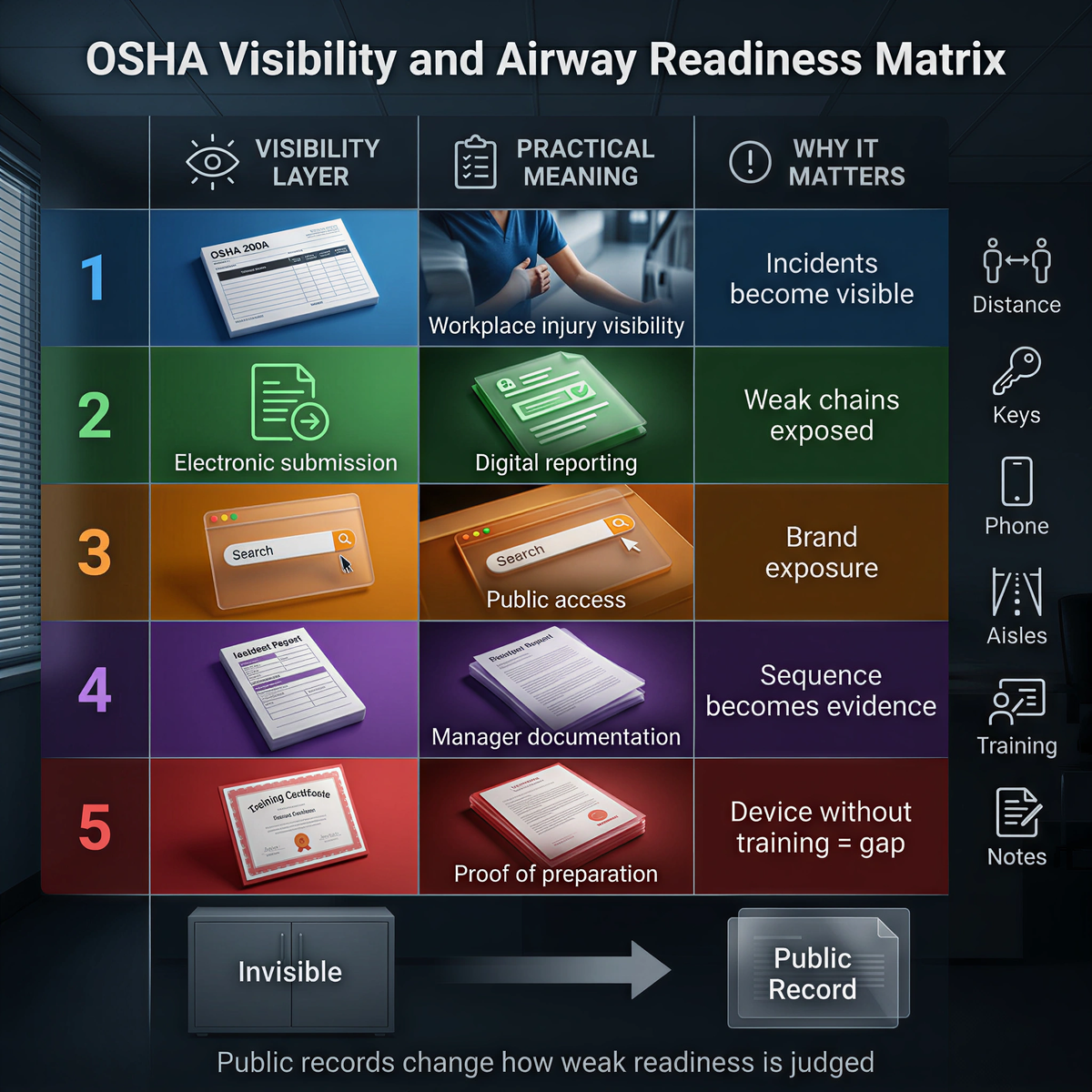
|
Visibility layer |
Practical meaning |
Why it matters for choking readiness |
|
OSHA 300A posting |
Workplace injury and illness visibility |
Leadership cannot treat serious incidents as invisible after the fact |
|
Electronic ITA submission |
Injury and illness data may move into a broader reporting environment |
Weak response-chain details may become easier to scrutinize |
|
Establishment search tools |
Public-facing access to inspection and record information |
Brand and litigation exposure can extend beyond the event |
|
Internal incident notes |
Managers document what happened and who acted |
The rescue sequence becomes evidence of preparation or delay |
|
Training records |
Proof of who was prepared to act |
A device purchase without role training leaves a visible gap |
Dense worksites lose time faster
Dense environments punish vague planning.
Noise hides early distress. Crowds block line of sight. Narrow aisles slow movement. A worker may be holding plates, pushing a cart, handling a register, or managing guests while the person choking is already losing air.
Severe choking often becomes quiet. Hearing contributes less than people expect. Physical reach becomes the controlling variable.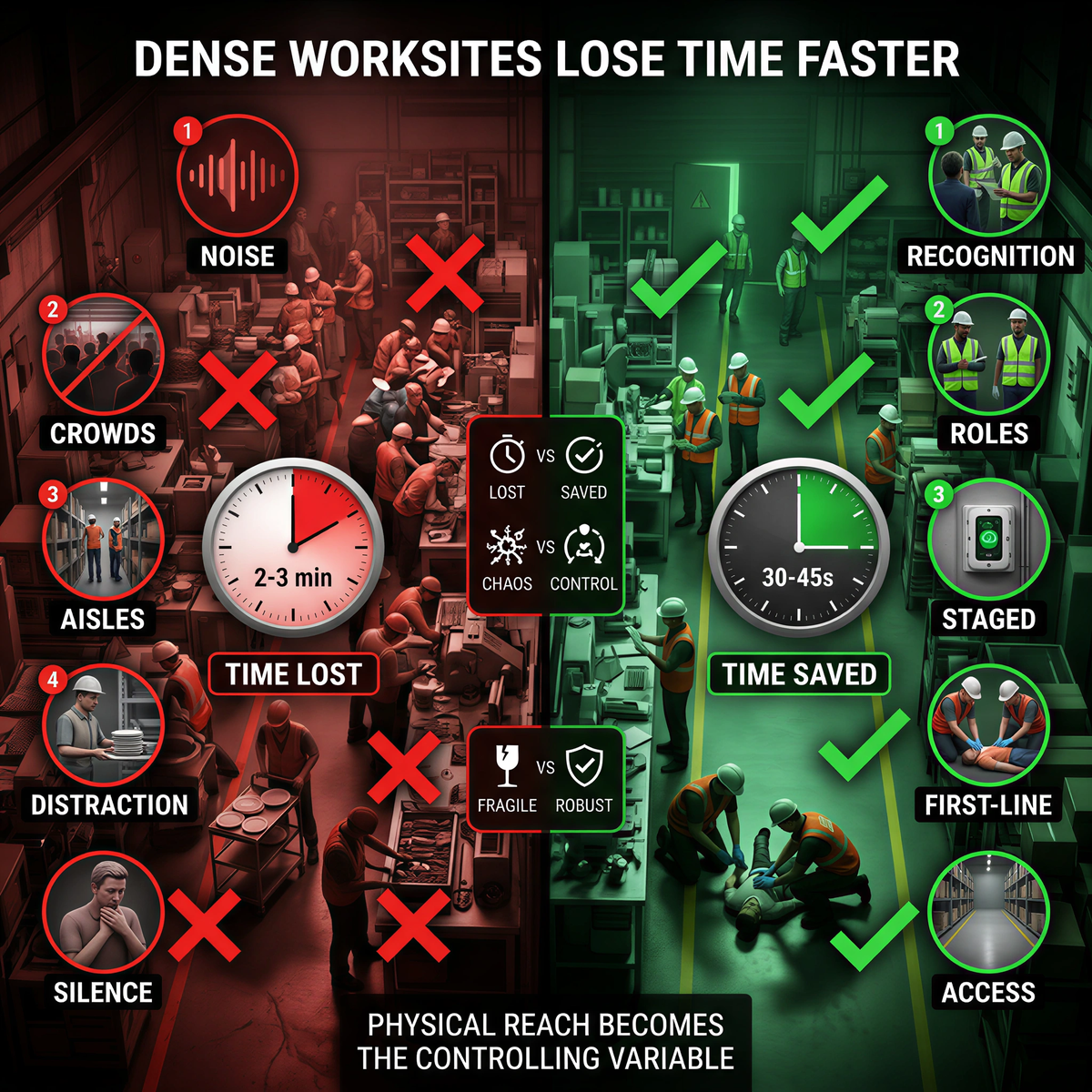
A choking rescue device for businesses, workplace choking emergency kit, or emergency airway suction device can support a broader plan only if it is placed where the emergency is likely to begin. A backup tool in a locked office may be technically owned but operationally absent.
A second-line airway response path is not a substitute for first-line choking rescue.
Manual choking first aid still anchors the event. 911 or local emergency services still need to be activated. CPR readiness still matters if the person becomes unresponsive.
The second-line question appears after first-line attempts have not resolved the obstruction. What can the room do next without abandoning the person?
A reachable FDA-authorized QXN suction anti-choking device can be one part of that answer when it is placed, labeled, trained, and used within its instructions. It is not proof of safety by itself. It is one physical redundancy layer inside a restaurant choking emergency plan or workplace airway safety program.
This is the correct boundary for restaurants, hotels, offices, and dense worksites. The device is not the plan. The plan is the sequence that gets the right action to the right place in time.

Walk the real floor during a busy period, not an empty morning inspection.
Start from the places where choking is most likely to begin.
Measure how long it takes to recognize severe choking, start first-line care, call 911, reach a trained responder, retrieve any second-line airway backup, clear space around the person, prepare for CPR if the person becomes unresponsive, and meet EMS at the correct entrance.
Then ask the uncomfortable question: does the first witness have to leave the person to find a phone, key, manager, or device?
If yes, the response path is already too fragile.
Many managers considering choking emergency equipment for restaurants, offices, hotels, or hospitality spaces are not asking only about price.
They are wondering whether employees will panic. They are asking whether the device creates liability. They are unsure whether it belongs in the dining room or the office. They are worried that buying one looks like admitting the hazard exists.
Those are practical concerns.
The weak answer is to buy a device and treat the purchase as the plan. The stronger answer is to map the floor, train the first witness, define the second-line step, and document why placement makes sense.
If the first responder must cross a crowded banquet room to reach the nearest backup tool, the safety plan has already timed out.
A stronger workplace airway plan does not need to be complicated. It needs to be usable.
It should include a severe choking recognition cue that staff can remember under stress.
It should define who stays with the person and who calls 911.
It should identify where backup resources are staged and how long retrieval takes.
It should make clear that second-line equipment does not replace first-line care.
It should assign a person to meet EMS.
It should require a short incident review after any serious event or near miss.
Most workplaces already know how to write safety policies. The harder work is making the policy behave in a full dining room, a loud banquet hall, a crowded break area, or a night-shift cafeteria when the first witness has ten seconds to make the room move.
For related planning context, review the anti-choking device buyer evidence checklist.
For related planning context, review the proof of safety.
No. A choking-specific standard is not required for workplace airway emergencies to matter. Employer duties can still be relevant when a recognized serious hazard exists and the site has not built a feasible response path.
OSHA posting, electronic reporting, establishment search tools, internal incident notes, and training records can make weak readiness more visible after a serious event. A vague policy is weaker than a documented response path.
It is the reachable backup route after first-line choking rescue does not clear the obstruction. It includes staff roles, 911 activation, retrieval route, visible staging, second-line equipment access, CPR readiness, and EMS handoff.
A restaurant may choose to stage an FDA-authorized suction anti-choking device as part of a second-line airway response plan. The purchase should not replace choking first-aid training, 911 activation, CPR readiness, or floor-level retrieval planning.
Placement should be based on reach-time from likely choking locations, not administrative convenience. Restaurants, hotels, offices, and factories should audit dining areas, break rooms, banquet zones, and employee meal spaces before choosing storage points.
Start with reach-time. If the first witness has to leave the person to find a phone, key, manager, or backup tool, the response path is too fragile.
A serious workplace incident can create records through internal reporting, training documentation, injury and illness reporting, inspection history, or legal review. The stronger the response documentation, the easier it is to show that the site planned beyond a generic first-aid statement.
OSHA General Duty Clause, Section 5 duties
OSHA Injury Tracking Application (ITA)
FDA Safety Communication, March 4, 2026
This article is for operational planning and educational purposes only. It does not constitute legal, OSHA, regulatory, or medical advice. Employers should review workplace-specific emergency planning, OSHA coverage, recordkeeping duties, and device use with qualified counsel, safety leadership, and medical or first-aid professionals.




















