LifeVac reviews can reveal buyer friction, reported use, and storage problems, but they cannot prove clinical effectiveness. Serious review analysis audits retrieval latency inside the first 4 minutes, product-specific FDA status, 21 CFR 874.5400, QXN labeling, pressure evidence, mask integrity, and first-line rescue sequence.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
People search for LifeVac reviews because they want the closest available signal of what happened outside a lab. A parent wants reassurance before placing a device in the kitchen. A school buyer wants to know whether staff can understand the instructions. An adult child caring for an older parent wants to know whether a second-line backup is worth staging near meals.
Review analytics must replace emotional consensus. Under stress, anecdotal reports do not dictate biological survival. They show experience, friction, perception, and sometimes field-use stories. They rarely provide a complete obstruction timeline, product identity, mask condition, EMS record, or medical follow-up.
The buyer's job is not to worship reviews or dismiss them. The job is to place reviews in the evidence stack: regulatory status, first-line protocol, bench performance, material condition, seller traceability, reported-use files, and the physical room where the device will be stored.
A public review can be sincere and incomplete at the same time. A person may report a dramatic rescue without knowing whether the airway was fully obstructed, whether the obstruction moved after back blows, whether vomiting contributed, whether the device sealed properly, or whether EMS documented the same sequence.
A five-star review is not a denominator. A one-star complaint is not a controlled failure analysis. Both can contain useful information. Neither should be read as a substitute for product-specific evidence.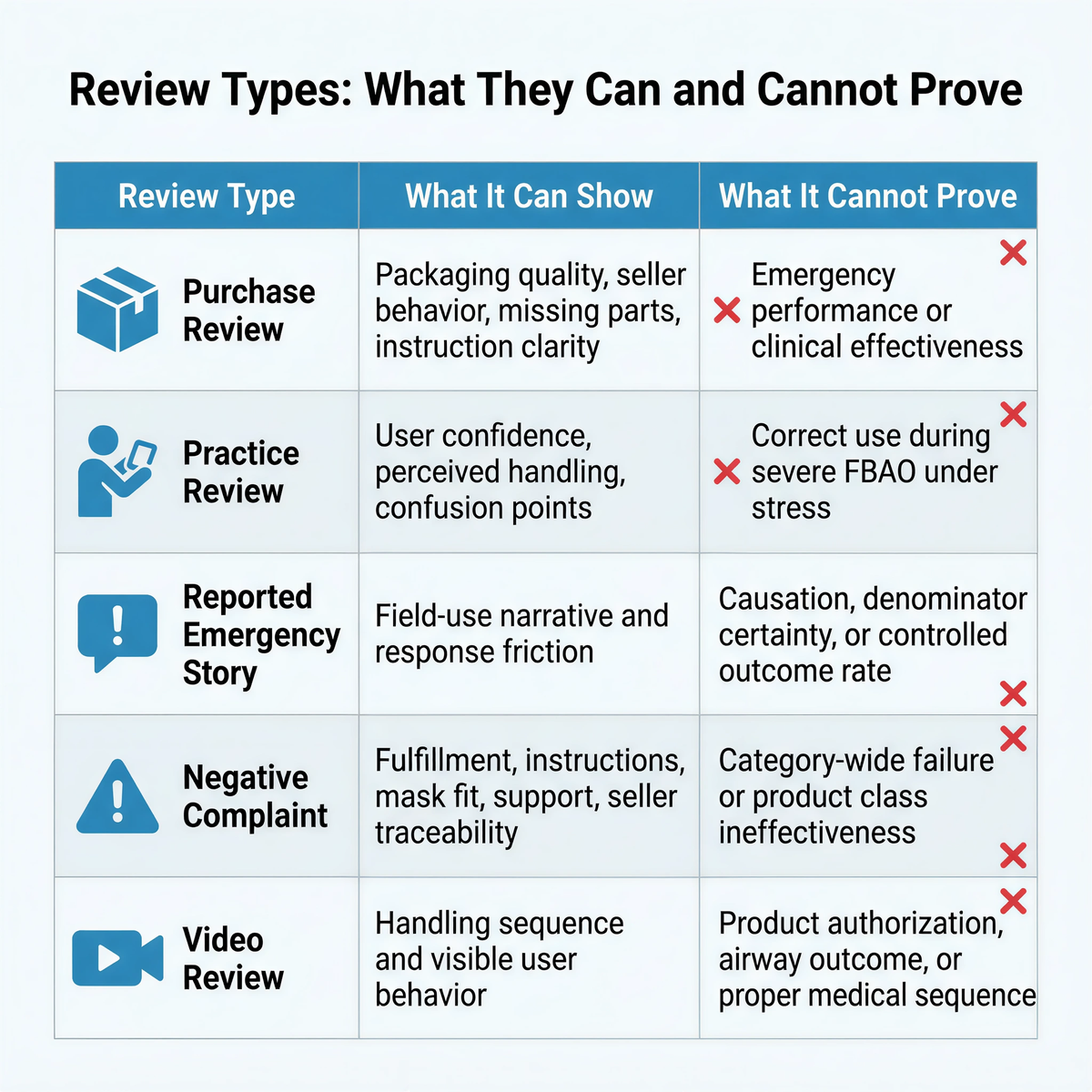
|
Review type |
What it can show |
What it cannot prove |
|
Purchase review |
Packaging quality, seller behavior, missing parts, instruction clarity. |
Emergency performance or clinical effectiveness. |
|
Practice review |
User confidence, perceived handling, confusion points. |
Correct use during severe FBAO under stress. |
|
Reported emergency story |
Field-use narrative and response friction. |
Causation, denominator certainty, or controlled outcome rate. |
|
Negative complaint |
Fulfillment, instructions, mask fit, support, seller traceability. |
Category-wide failure or product class ineffectiveness. |
|
Video review |
Handling sequence and visible user behavior. |
Product authorization, airway outcome, or proper medical sequence. |
Reviews should never move the device ahead of first-line choking rescue. For responsive adults and children with severe foreign-body airway obstruction, current first-line rescue uses repeated cycles of 5 back blows and 5 abdominal thrusts. When abdominal thrusts are not feasible because of pregnancy, severe obesity, body geometry, or other physical limits, chest thrusts may replace abdominal thrusts. Infants follow a separate sequence of 5 back blows and 5 chest thrusts, not abdominal thrusts.
A suction device belongs after standard measures are unsuccessful and only within product-specific instructions. FDA's 2026 second-line framework under 21 CFR 874.5400 and product code QXN reinforces that boundary. A review describing device-first use may still be a real review, but it does not define the correct rescue sequence.
The useful question is not whether reviews sound convincing. The useful question is whether they identify a response delay, a product failure point, or an evidence gap.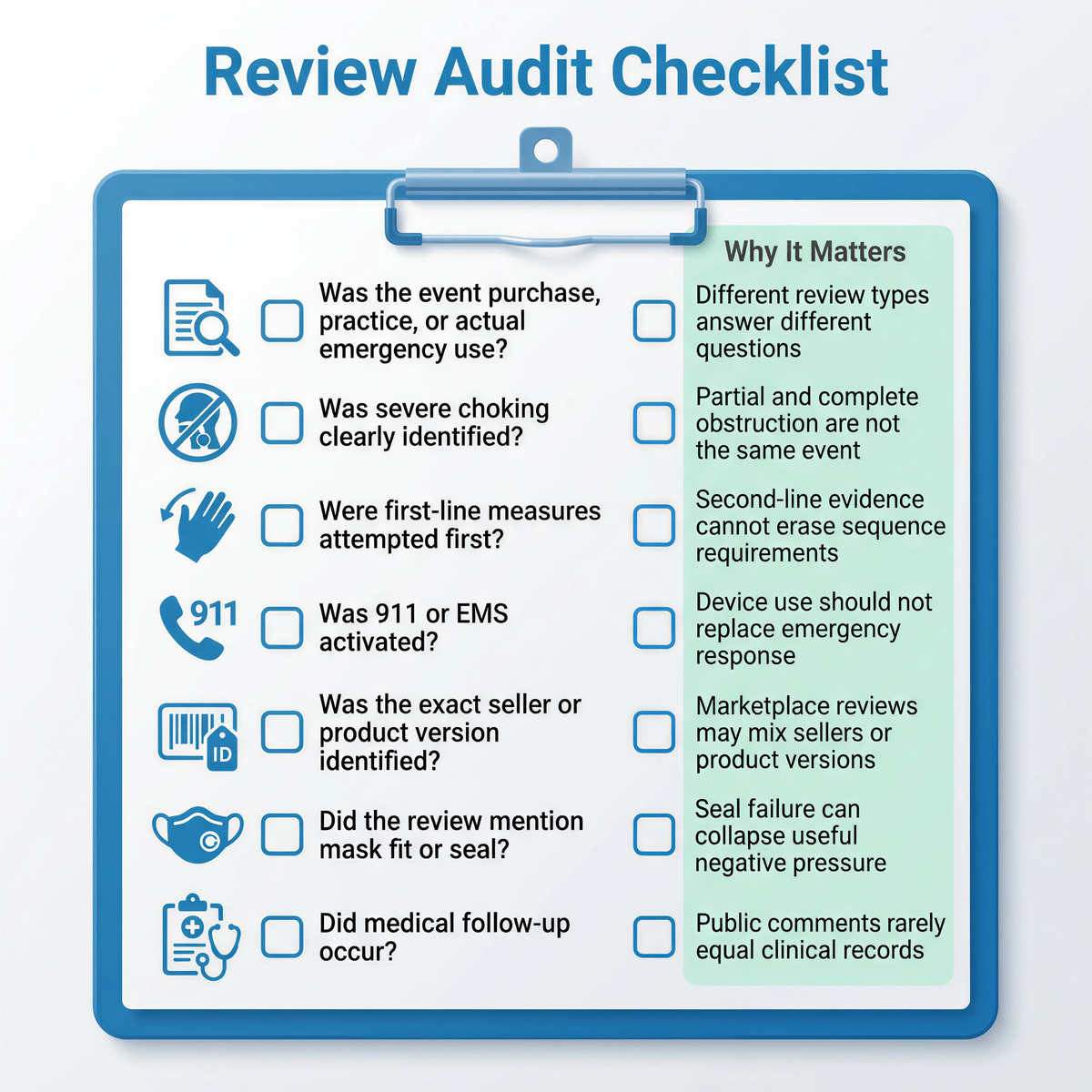
|
Review audit question |
Why it matters |
|
Was the event purchase, practice, or actual emergency use? |
Different review types answer different questions. |
|
Was severe choking clearly identified? |
Partial obstruction and complete obstruction are not the same event. |
|
Were first-line measures attempted first? |
Second-line evidence cannot erase sequence requirements. |
|
Was 911 or EMS activated? |
Device use should not replace emergency response. |
|
Was the exact seller or product version identified? |
Marketplace reviews may mix sellers or product versions. |
|
Did the review mention mask fit or seal? |
Seal failure can collapse useful negative pressure. |
|
Did medical follow-up occur? |
Public comments rarely equal clinical records. |
Families often trust reported rescues because the physical event is easy to imagine: food blocks the airway, manual rescue fails, a device is used, the person recovers. The real mechanics are less tidy.
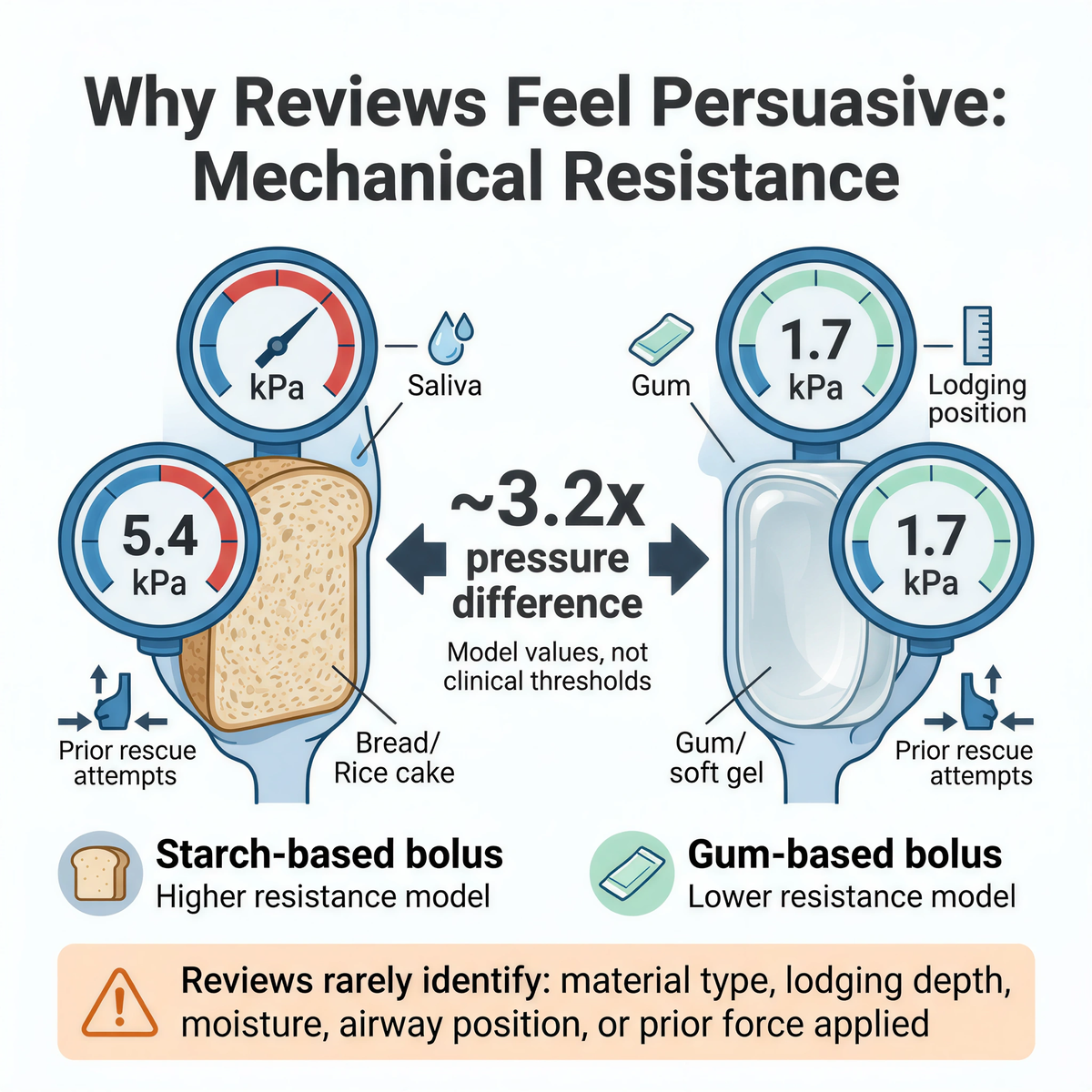
Experimental oral-flow work has reported model clearing pressures around 5.4 kPa for starch-based material and about 1.7 kPa for gum-based material of similar apparent viscosity. Those values are not clinical thresholds for suction-device success. They show a narrower engineering truth: obstruction material changes the resistance problem by roughly 3.2 times in the tested model.
A bread bolus, rice cake, meat piece, grape, nut, soft gel, saliva-wet food, denture-related geometry, and delayed recognition do not create the same event. A review rarely identifies material, lodging depth, moisture, airway position, or the force already applied during first-line rescue.
|
Obstruction variable |
Why reviews usually miss it |
Why engineering teams still care |
|
Food material |
Reviews often say "food" without specifying bolus type. |
Starch-based material may require much higher model-clearing pressure than gum-like material. |
|
Moisture and saliva |
Field stories rarely define surface lubrication. |
Adhesion and deformation change how a bolus moves. |
|
Lodging geometry |
Public comments rarely identify vocal-fold level or pharyngeal position. |
Depth and shape change removal mechanics. |
|
Prior first-line actions |
Reviews may not separate back blows, thrusts, coughing, vomiting, or device use. |
Outcome attribution becomes uncertain. |
|
Mask seal |
Buyers may not notice micro-leak paths. |
Leak paths collapse pressure gradients during pull. |
Marketplace reviews can be dangerous when seller identity is weak. A review attached to a product page may not refer to the same product version, same seller, same valve geometry, same mask material, or same instructions currently being sold.
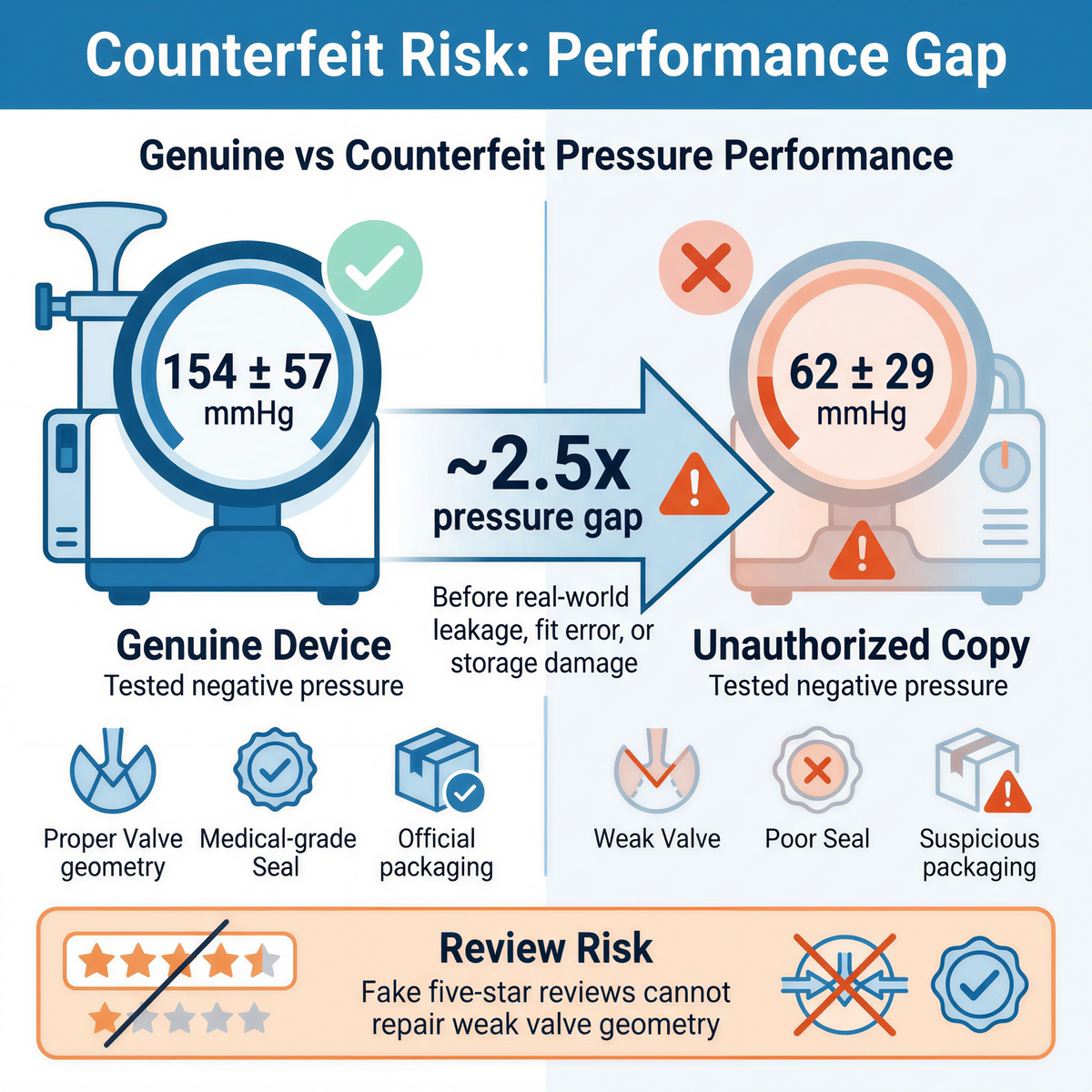
A 2025 comparative bench study reported about 154 +/- 57 mmHg negative pressure from a genuine device and about 62 +/- 29 mmHg from an unauthorized copy in the tested setup. The lower-pressure copy was not merely a cheaper legal problem. It was a performance problem: roughly a 2.5-fold negative-pressure gap before real-world leakage, fit error, storage damage, or user motion entered the event.
Fake five-star reviews cannot repair weak valve geometry. A positive marketplace rating cannot prove one-way airflow, seal integrity, mask material, or current FDA status.
|
Marketplace signal |
Risk if misread |
Buyer action |
|
High star rating |
May reflect price, shipping, or perceived value rather than performance. |
Verify seller, instructions, product identity, and replacement path. |
|
Generic "works great" comments |
May not describe emergency use or exact product. |
Look for detailed use context and traceability. |
|
Copied images or vague brand language |
May hide unauthorized copies or old claims. |
Confirm official channel and product documentation. |
|
"FDA registered" claim |
Can be mistaken for product authorization. |
Check exact product status and category language. |
|
Low price plus urgent safety claim |
Can pull buyers toward unsupported listings. |
Audit valve, mask, materials, IFU, and seller source. |
Some reviews involve the users most likely to challenge a simple product story: older adults, wheelchair users, people with dentures, people with dysphagia, children with neurologic impairment, and medically complex pediatric patients.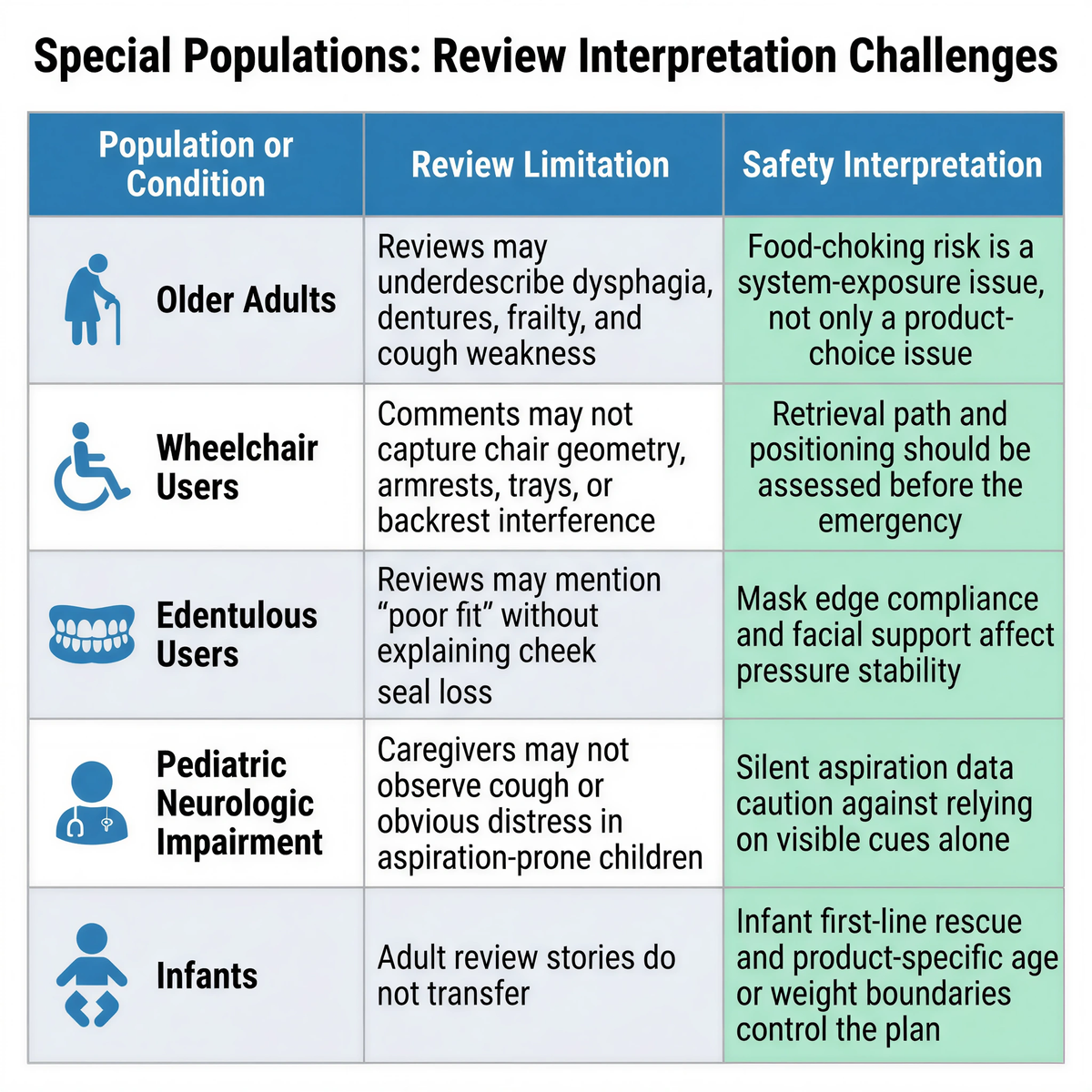
Published geriatric swallowing literature has reported that adults over 65 can face food-choking incidence around seven times higher than children aged 1 to 4. Pediatric aspiration literature also shows why observation can fail: in one high-risk pediatric aspiration cohort, thin fluids were silently aspirated in 81% of aspirating patients. The relevant lesson is not that those data prove suction-device performance. They show that visual observation, family memory, and review narratives can miss the airway event's real physiology.
|
Population or condition |
Review limitation |
Safety interpretation |
|
Older adults |
Reviews may underdescribe dysphagia, dentures, frailty, and cough weakness. |
Food-choking risk is a system-exposure issue, not only a product-choice issue. |
|
Wheelchair users |
Comments may not capture chair geometry, armrests, trays, or backrest interference. |
Retrieval path and positioning should be assessed before the emergency. |
|
Edentulous users |
Reviews may mention "poor fit" without explaining cheek collapse or seal loss. |
Mask edge compliance and facial support affect pressure stability. |
|
Pediatric neurologic impairment |
Caregivers may not observe cough or obvious distress in aspiration-prone children. |
Silent aspiration data caution against relying on visible cues alone. |
|
Infants |
Adult review stories do not transfer. |
Infant first-line rescue and product-specific age or weight boundaries control the plan. |

A mask can appear clean and still lose mechanical function. Silicone material behavior is not judged only by color or surface cleanliness. Shore A hardness, elongation at break, edge recovery, surface tack, and storage deformation all affect the seal.
Medical-grade silicone can still change over time, especially after contact with skin oils, heat cycles, cleaning agents, pressure deformation, or repeated handling. Aging can increase Shore A hardness, reduce elasticity, lower elongation at break, and reduce edge compliance. During a fast pull, a stiffened mask edge may not follow edentulous cheeks, facial hair, uneven anatomy, or a moving jaw. The result is a micro leak path and a rapid pressure-gradient collapse.
A review saying the mask "looked fine" does not answer the mechanical question. Mask replacement and inspection schedules belong in the readiness file, not in memory.
|
Mask condition factor |
What changes physically |
Why reviews may miss it |
|
Shore A hardness |
Higher hardness means greater resistance to local deformation. |
The mask may still look normal. |
|
Elongation at break |
Lower elongation reduces stretch reserve. |
Buyers rarely test stretch or edge recovery. |
|
Edge compliance |
Stiffer edges fail to follow facial geometry. |
Leak paths may occur only during a pull. |
|
Surface contamination |
Skin oil or cleaner residue can change contact behavior. |
A clean-looking surface can still seal poorly. |
|
Storage deformation |
Compressed masks can retain shape memory. |
Packaging may hide deformation until use. |
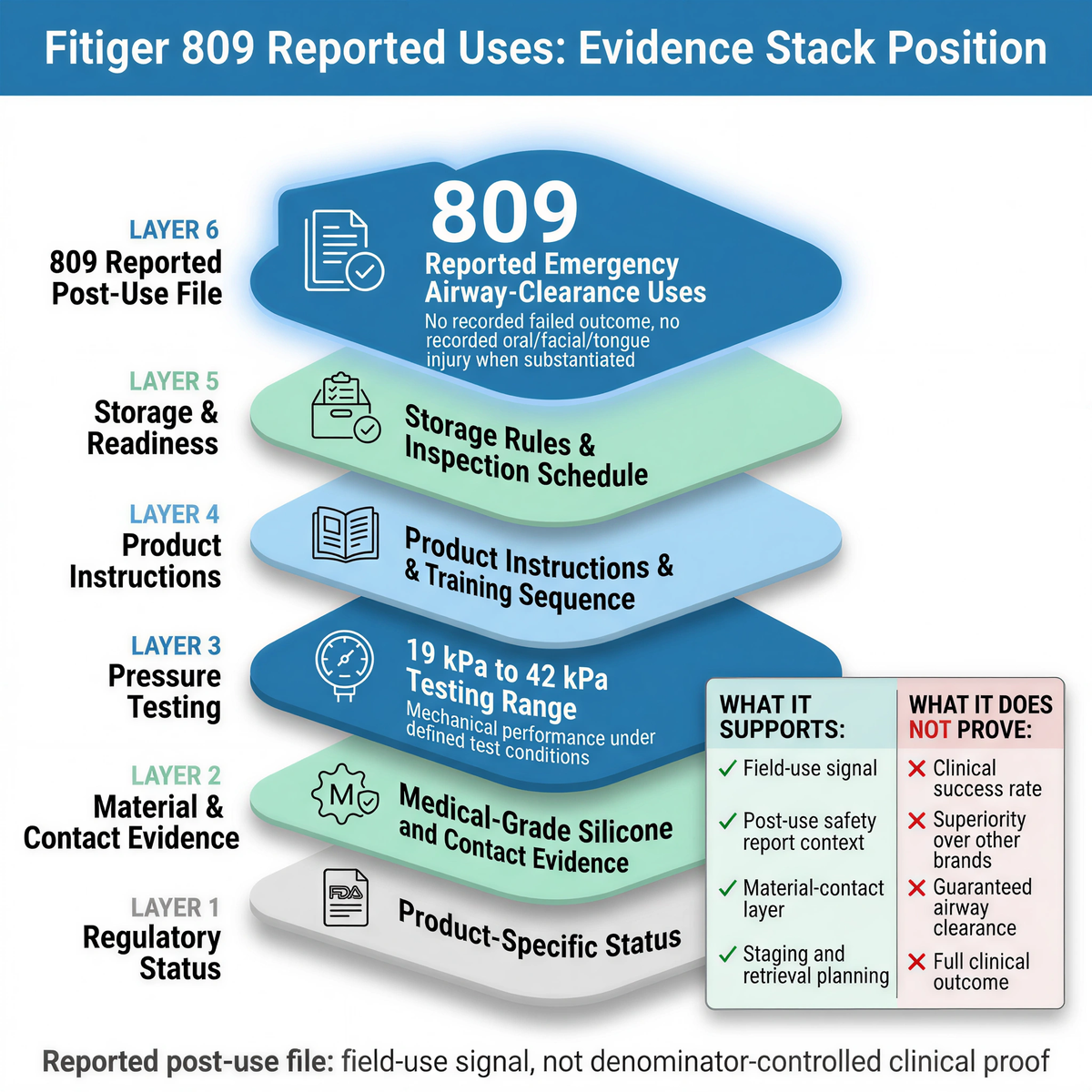
Fitiger has referenced 809 reported emergency airway-clearance uses, with no recorded failed outcome and no recorded oral, facial, or tongue injury report when substantiated at the time of publication. That record belongs in the evidence stack. It should not be inflated into a randomized clinical trial, a universal success rate, or proof of clinical superiority over LifeVac, Dechoker, or any other brand.
The disciplined label is reported post-use file. It is a field-use signal, not denominator-controlled clinical proof. It becomes more useful when read beside pressure testing, material-contact evidence, product instructions, storage rules, training sequence, and seller traceability.
|
Fitiger evidence layer |
What it supports |
What it does not prove |
|
809 reported post-use file |
Field-use signal and post-use safety report context. |
Clinical success rate or superiority. |
|
Mechanical performance under defined test conditions. |
Guaranteed airway clearance. |
|
|
Medical-grade silicone and contact evidence |
Material-contact layer and mask evaluation. |
Full clinical outcome. |
|
Staging and retrieval-latency planning. |
Rescue success by itself. |
|
|
EasyPumpVac short operation path |
Reduced handling burden after first-line failure. |
Correct use without training or instructions. |
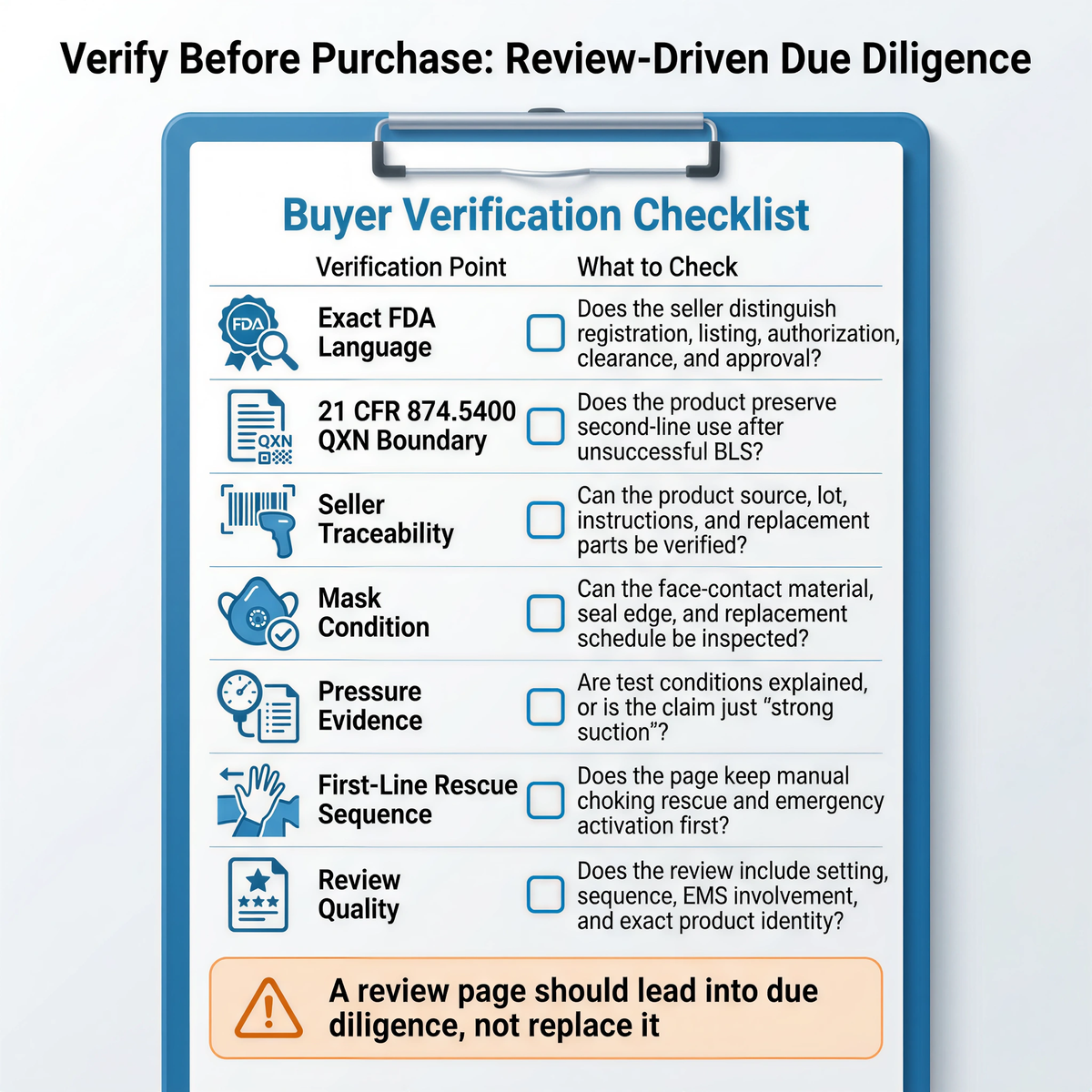
A review page should lead into due diligence, not replace it.
|
Verification point |
What to check before purchase |
|
Exact FDA language |
Does the seller distinguish registration, listing, authorization, clearance, and approval? |
|
21 CFR 874.5400 / QXN boundary |
Does the product preserve second-line use after unsuccessful BLS? |
|
Seller traceability |
Can the product source, lot, instructions, and replacement parts be verified? |
|
Mask condition |
Can the face-contact material, seal edge, and replacement schedule be inspected? |
|
Pressure evidence |
Are test conditions explained, or is the claim just "strong suction"? |
|
First-line rescue sequence |
Does the page keep manual choking rescue and emergency activation first? |
|
Review quality |
Does the review include setting, sequence, EMS involvement, and exact product identity? |
Fitiger should not try to win a review query by attacking LifeVac reviews. The stronger position is stricter: reviews are useful but insufficient; reported-use files matter but are not trials; bench evidence matters but is not a rescue guarantee; mask materials matter but must be inspected; FDA status matters only when it is product-specific; first-line rescue remains first.
Fitiger belongs in the review conversation when buyers want more than emotional consensus: reported post-use context, pressure-testing boundaries, material-contact evidence, storage readiness, FoldPumpVac portability, EasyPumpVac short operation path, and second-line positioning after unsuccessful standard measures.
|
Question |
Reason |
|
Is this purchase, practice, or emergency use? |
Each review type answers a different evidence question. |
|
Does it describe severe choking signs? |
Partial and complete obstruction cannot be merged. |
|
Does it mention first-line rescue? |
The second-line boundary depends on sequence. |
|
Was EMS called or medical follow-up documented? |
Outcome claims need clinical context. |
|
Is the exact product and seller identified? |
Copycat listings can contaminate review interpretation. |
|
Does the review mention mask fit or seal? |
Seal failure is a major pneumatic failure path. |
|
Does it overclaim a guaranteed rescue? |
Guarantee language is marketing, not evidence. |
For related planning context, review the 21 CFR 874.5400.
No. Reviews can show buyer experience, perceived ease of use, packaging quality, instruction clarity, and reported field stories. They cannot prove controlled clinical effectiveness or clinical superiority.
No. Reviews can be useful when read as one evidence layer beside FDA status, instructions, bench testing, material evidence, seller traceability, and first-line rescue guidance.
A silicone mask can look clean while its Shore A hardness, edge compliance, elongation, or surface contact behavior has changed. Stiffer mask edges can create leak paths during a fast pull, especially on edentulous or irregular facial geometry.
Fitiger should describe the 809 figure as a reported post-use file, not as randomized clinical proof. It is a field-use signal that should be read with pressure testing, material-contact evidence, instructions, and regulatory status.
Reviews may not identify the exact seller or product version. Device identity matters because pressure, valve direction, mask material, instructions, and traceability can differ between genuine and unauthorized copy products.
Useful reviews describe the setting, sequence, first-line measures, emergency activation, exact product, seller source, mask fit, and medical follow-up. Short emotional reviews may be sincere but incomplete.
|
Source Name |
What it Supports |
Full URL |
|
FDA Safety Communication, March 4, 2026 |
Supports the first-line-first and second-option framing for anti-choking devices. |
|
|
FDA De Novo Order DEN250012 |
Supports 21 CFR 874.5400, product code QXN, and second-line suction anti-choking device classification language. |
https://www.accessdata.fda.gov/cdrh_docs/pdf25/DEN250012.pdf |
|
FDA Registration and Listing Reminder |
Supports the statement that registration and listing do not denote approval, clearance, or authorization. |
|
|
American Heart Association 2025 Adult FBAO Algorithm |
Supports repeated cycles of 5 back blows followed by 5 abdominal thrusts for responsive adults with severe FBAO. |
|
|
American Heart Association 2025 Child FBAO Algorithm |
Supports repeated cycles of 5 back blows followed by 5 abdominal thrusts for responsive children with severe FBAO. |
|
|
Comparative bench pressure study, 2025 |
Supports the 154 +/- 57 mmHg versus 62 +/- 29 mmHg negative-pressure comparison between a genuine device and an unauthorized copy under tested conditions. |
|
|
Velayutham et al., Silent Aspiration: Who Is at Risk? |
Supports pediatric silent aspiration discussion, including high silent aspiration rates among aspirating patients in the studied cohort. |
|
|
Cichero, Age-Related Changes to Eating and Swallowing Impact Frailty |
Supports the discussion of older-adult food choking risk and age-related swallowing vulnerability. |
|
|
Food Oral Processing and Tribology review |
Supports the 5.4 kPa versus 1.7 kPa model comparison for different bolus materials under tested conditions. |
|
|
MedlinePlus CPR Reference |
Supports the operational importance of the early oxygen window in non-breathing emergencies. |
LifeVac is mentioned only for identification and comparison. LifeVac and other product names are trademarks of their respective owners. This article is an independent Fitiger buyer-education guide. It compares review signals, evidence boundaries, response-sequence requirements, and Fitiger's own reporting limits. It does not claim that any product is clinically superior unless product-specific, comparable evidence directly supports that claim.
This article is for preparedness, engineering, product-safety, and evidence-interpretation purposes only. It is not medical, legal, or regulatory advice. In a choking emergency, follow established first-line rescue protocols, call 911 or local emergency services, and treat suction anti-choking devices only as second-line options after unsuccessful standard choking rescue measures, consistent with current FDA public guidance and product-specific instructions.




















