Remote airway readiness fails when placement follows the building instead of the route. OSHA still reads life-threatening first-aid access around a 3-4 minute window. Rural EMS chains often run far beyond that. FDA's 2026 second-line framework only works when the backup layer sits inside reach, inside sequence, and inside the real delay pattern of the moving scene.
A lot of deployments still start with the wrong map.
The first-aid cabinet goes in the admin office. The airway backup device goes in the nurse room. The depot wall station goes near the main entrance. The route vehicle gets whatever fits in the trunk.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
That looks organized. It often produces the wrong response geometry.
A worker in a remote loading lane is not standing where the office is. A driver thirty miles into a route is not protected by the cabinet in the base building. A bus aide managing a medically fragile student does not have time to translate a campus floor plan into a moving response path. Placement logic has to follow the scene that will actually fail, not the room that looks easiest to document.
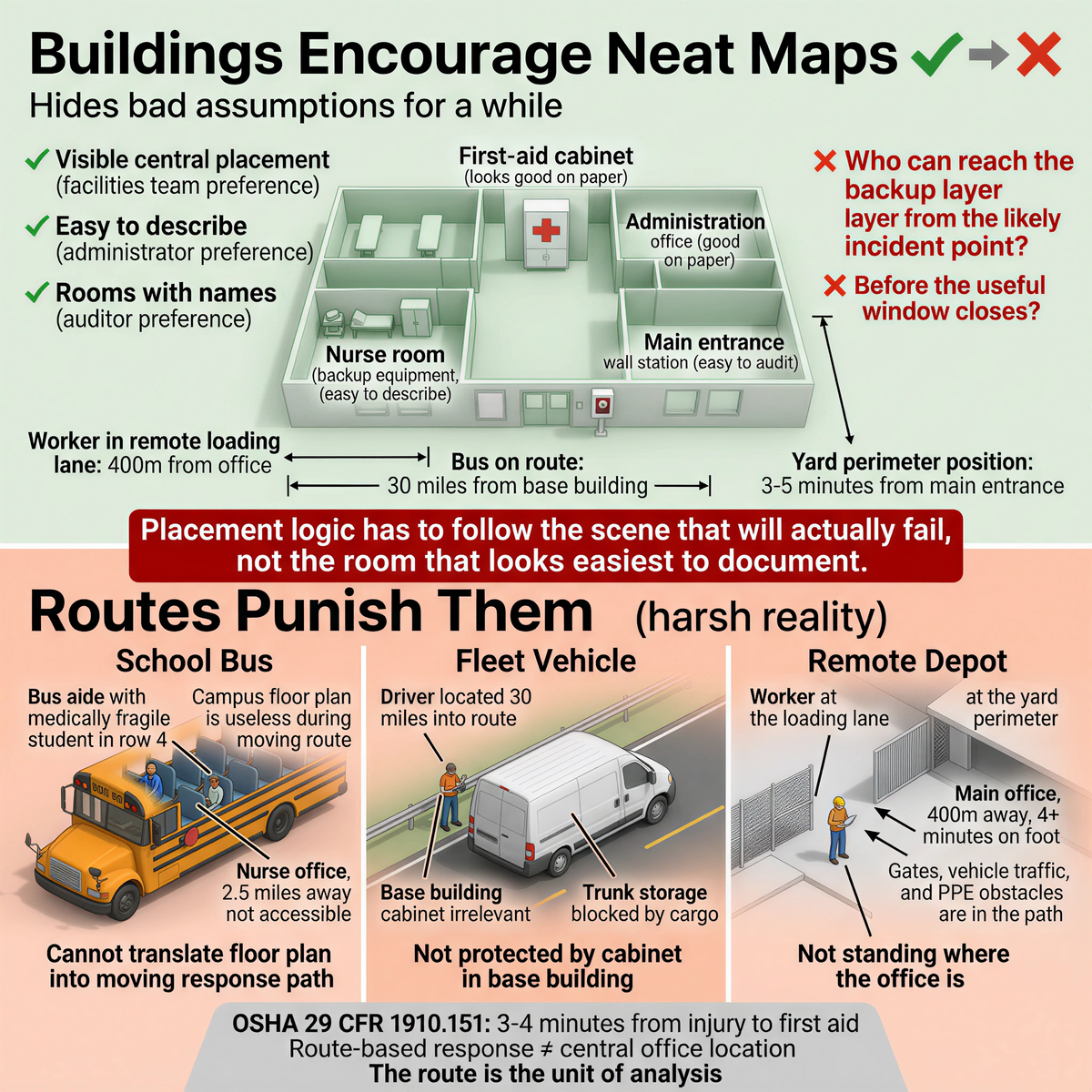
A building hides bad assumptions for a while. A route exposes them fast.
Facilities teams like visible central placement. Administrators like locations that are easy to describe. Auditors like rooms with names. None of those preferences answer the operational question that matters:
Who can reach the backup layer from the likely incident point before the useful window closes?
OSHA's interpretation of 29 CFR 1910.151 keeps that window short when suffocation, stopped breathing, or other life-threatening injuries are possible. The agency has repeatedly interpreted 'near proximity' around 3 to 4 minutes from injury to first aid. A route-based response system that assumes a central office location still qualifies as near because it belongs to the same employer is not reading the standard the way OSHA reads it.
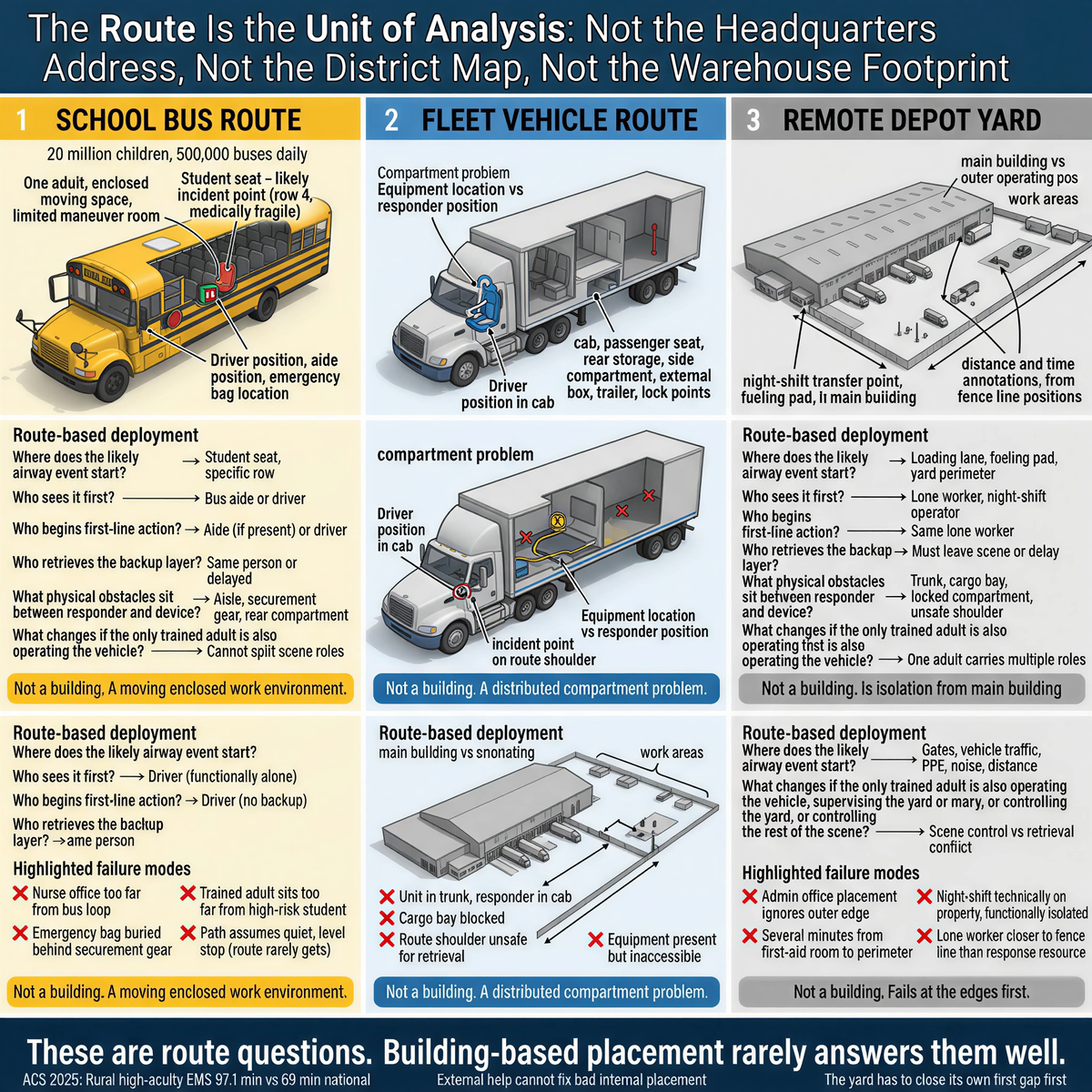
A bus is not a building. A long-haul truck is not a building. A yard tractor, a fuel route, a field-service van, and a remote transfer point are not smaller versions of a building.
They are moving or distributed work environments with different incident points, different access paths, different responder pools, and different EMS assumptions.
Fitiger's engineering and product safety view treats the route as the unit that has to be audited. Not the headquarters address. Not the district map. Not the warehouse footprint. The route.
That changes the deployment questions immediately:
Those are route questions. Building-based placement rarely answers them well.
The FDA's March 4, 2026 De Novo order DEN250012 created 21 CFR 874.5400 for a 'suction anti-choking device as a second-line treatment.' The category is Class II, product code QXN, and is limited to complete airway obstruction after unsuccessful use of a BLS choking protocol. That made the backup layer easier to define. It did not make placement mistakes less dangerous.
A lawful second-line device placed in the wrong spot still enters too late.
Packaging latency is a fatal variable. In rural transport, a second-line tool hidden in a rear compartment, stored in the wrong room, or staged at the wrong end of the route adds seconds to an oxygen window that is already nearly gone. Placement is not a storage decision. It is a timing decision.
Remote yards and logistics depots often look covered when the plan is drawn from the main office outward.
The far edge of the yard tells a different story.
A loading lane at the perimeter may be several minutes away from the first-aid room. A night-shift transfer point may be technically on the same property and functionally isolated. A lone worker at a fueling pad may be closer to the fence line than to any meaningful response resource. The distance is not theoretical once you time it on foot with gates, vehicle traffic, PPE, and noise in the way.
ACS reported in 2025 that high-acuity rural EMS activations averaged 97.1 minutes compared with 69 minutes nationally. That 28.1-minute absolute difference makes one point brutally clear: external help cannot be treated as the layer that fixes bad internal placement. The yard has to close its own first gap first.
A strong placement model for a remote depot usually starts at the outer operating positions, not the main building. The admin office may keep the records. The operational layer still has to move physically closer to the work.
A school bus route has almost no patience for abstract placement.
The national school bus safety action plan released in 2026 put the system's scale in plain view: about 20 million children riding about 500,000 buses every school day. A bus is an enclosed moving space with one adult more often than not, limited room to maneuver, limited leverage for manual intervention, and route-dependent EMS access. Conventional bus safety standards prioritize kinetic impact and crash survivability. Internal biological risk moves on a different clock.
Medically fragile routes tighten the logic further. A student with tracheostomy-related needs, aspiration risk, or higher airway vulnerability changes the route before the wheels move. The physically relevant placement question is not 'Is the district covered?' It is 'Where is the support layer relative to the student, the aide, the driver, and the stop-and-respond sequence on this exact bus?'
A route-based audit often produces uncomfortable answers:
- the nurse office is too far from the bus loop to matter
- the emergency bag is technically on board but buried behind securement gear
- the trained adult sits too far from the student most likely to expose the weakness first
- the path to the backup layer assumes a quiet, level stop that the route rarely gets
Those are placement failures, not training failures.
A lot of fleet readiness fails inside the vehicle itself.
The unit is in the trunk. The responder is in the cab. The route shoulder is unsafe. The cargo bay is blocked. The equipment is present and inaccessible.
A route vehicle has its own internal map: cab, passenger seat, rear storage, side compartment, external box, trailer access, lock points. A placement decision that ignores those internal compartments is still building-first thinking, just on a smaller scale.
The right question is not 'Is the unit on the vehicle?' The right question is 'Can the responder reach it from the event position without losing sequence integrity?'
That becomes sharper when the responder is alone. Lone drivers do not get to split the scene between one person doing first-line action and another doing retrieval. Placement has to account for one adult carrying more than one role.
Fitiger's audit method stays intentionally blunt.
If the route to the backup layer is longer than the sequence can tolerate, the placement is wrong.
That does not always mean the unit belongs closer to the likely incident point. Sometimes the route design itself needs to change. Sometimes the staffing model is the real problem. Sometimes a fixed building location should remain for records and replenishment while a smaller operational layer moves out to the bus, vehicle, or remote work position.
The route should be tested with a timer, not defended with a diagram.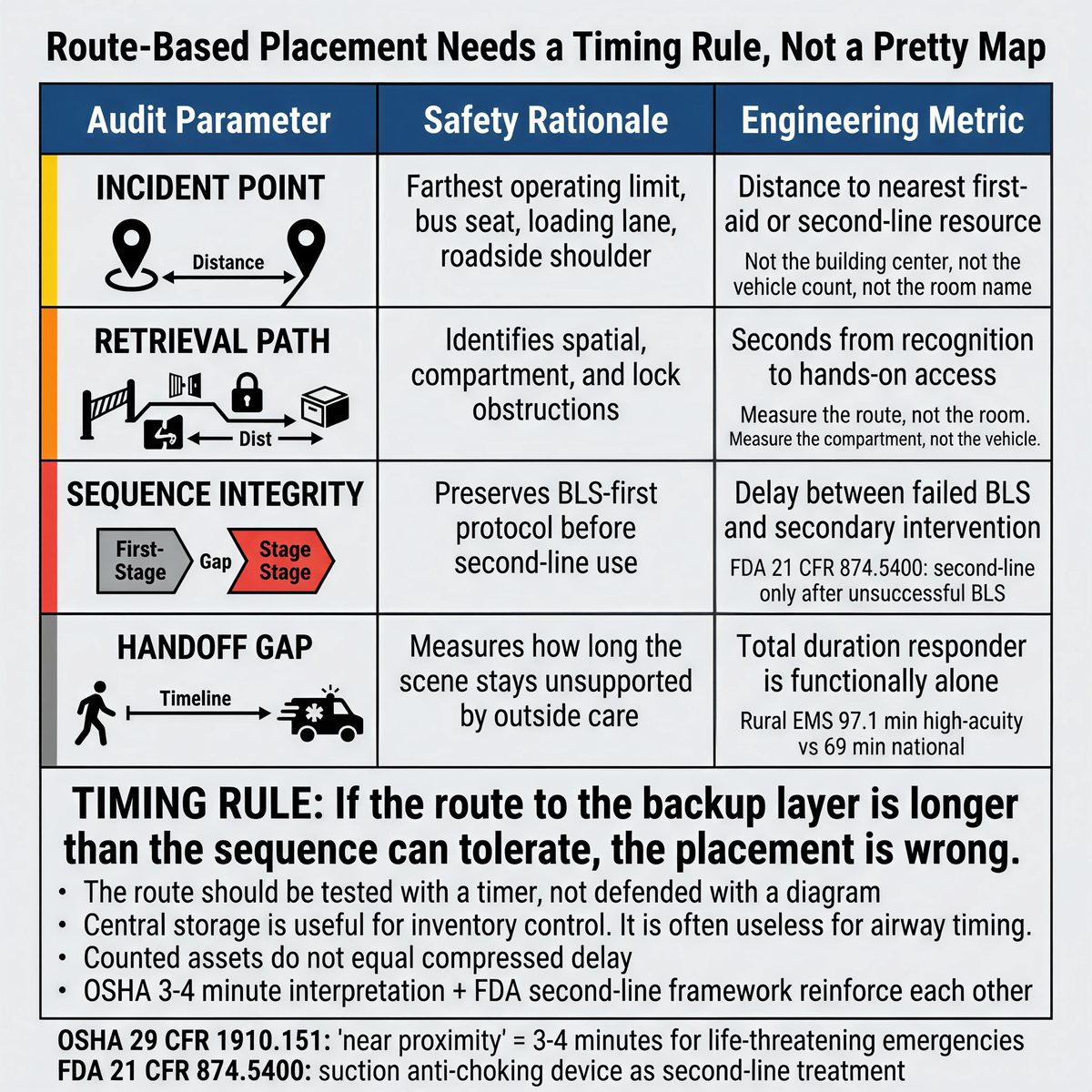
|
Audit Parameter |
Safety Rationale |
Engineering Metric |
|
Incident Point |
Farthest operating limit, bus seat, loading lane, roadside shoulder |
Distance to nearest first-aid or second-line resource |
|
Retrieval Path |
Identifies spatial, compartment, and lock obstructions |
Seconds from recognition to hands-on access |
|
Sequence Integrity |
Preserves BLS-first protocol before second-line use |
Delay between failed BLS and secondary intervention |
|
Handoff Gap |
Measures how long the scene stays unsupported by outside care |
Total duration responder is functionally alone |
Central storage is useful for inventory control. It is often useless for airway timing.
This is one of the most common gaps in rural and mobile systems. The employer can prove the equipment exists. The scene still cannot get to it inside the useful window. OSHA's 3-4 minute interpretation and the FDA's second-line framework reinforce each other. One keeps first aid physically close when the risk is life-threatening. The other defines the backup layer narrowly enough that bad placement can no longer hide behind generic product language. Counted assets do not equal compressed delay.
Do not start with the catalog.
Walk the route. Stand at the likely incident point. Time how long first-line action begins. Time how long the backup layer takes to reach the responder's hands. Measure the route, not the room name. Measure the compartment, not the vehicle count. Measure the far edge of the yard, not the building center.
Then ask the question central placement avoids:
Which deployment point actually closes the first dangerous gap?
If the answer is not the current location, move the location before you expand the inventory.
Pick one bus, one fleet vehicle, and one remote yard position this week.
Run the same test in all three:
- where would the event most likely start
- who would act first
- where is the backup layer now
- how many seconds does that route really take
Then compare the three paths.
The slowest path is the one your current map is lying about.
Download the Remote & Mobile Readiness Toolkit
When help may be minutes away, readiness has to be planned before the emergency.
Download the Remote & Mobile Airway Safety Readiness Toolkit to map delays, assign roles, plan equipment access, and prepare your team for choking emergencies in rural, mobile, or field-based environments.
Because a device that exists in the building may still be too far from the actual incident point. In airway emergencies, retrieval delay matters more than inventory visibility.
OSHA's long-standing interpretation of life-threatening first-aid access keeps the useful window around 3 to 4 minutes. That makes route-based access more important than simple building ownership.
The FDA created a defined second-line category for suction anti-choking devices under DEN250012. That made the backup layer easier to specify, but it still must be placed so it can enter the sequence in time.
A bus is a moving enclosed system with one adult, limited leverage, and route-dependent EMS access. A support layer staged in the wrong building is not a support layer for the bus at all.
Measure where the event would likely start, who would respond first, how long retrieval takes, and how long the responder is functionally alone before outside care becomes real.
OSHA interpretation letter, March 23, 2007
FDA De Novo Summary DEN250012
FDA Safety Communication, March 4, 2026
American College of Surgeons 2025 Rural EMS Study
National School Bus Safety Action Plan 2026
This article is for educational and operational planning purposes only. It does not provide medical or legal advice. Always follow current American Heart Association or Red Cross choking-response guidance, applicable OSHA requirements, local policy, and manufacturer instructions. In any real emergency, call 911 and begin trained first-line response immediately.




















