School choking safety equipment only helps if it is close, unlocked, and paired with trained staff. A real school choking emergency plan starts with recognition, 911 delegation, and 5 back blows plus 5 abdominal thrusts for responsive students over age 1. FDA-authorized QXN devices belong only as second-line backup after manual first aid fails.
A district can buy a school choking rescue device and still leave the cafeteria unprotected. That sounds harsh until you picture the scene. Lunch trays are clattering, a student is sitting near the end of a table, a cafeteria monitor notices the child suddenly stop talking, and the nurse's office is two corridors away behind a locked door. On paper, the campus owns choking safety equipment. In the first minute, the equipment may as well be across town.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
For meal-service teams, Fitiger's restaurant choking readiness plan gives practical guidance for staff roles, kit placement, and service-area response.
School administrators, nurses, cafeteria staff, coaches, and parents need a more honest conversation. The question is not only whether a school owns an anti choking device, choking rescue device, or airway clearance device. The question is whether the response can reach the student before the oxygen window starts closing.
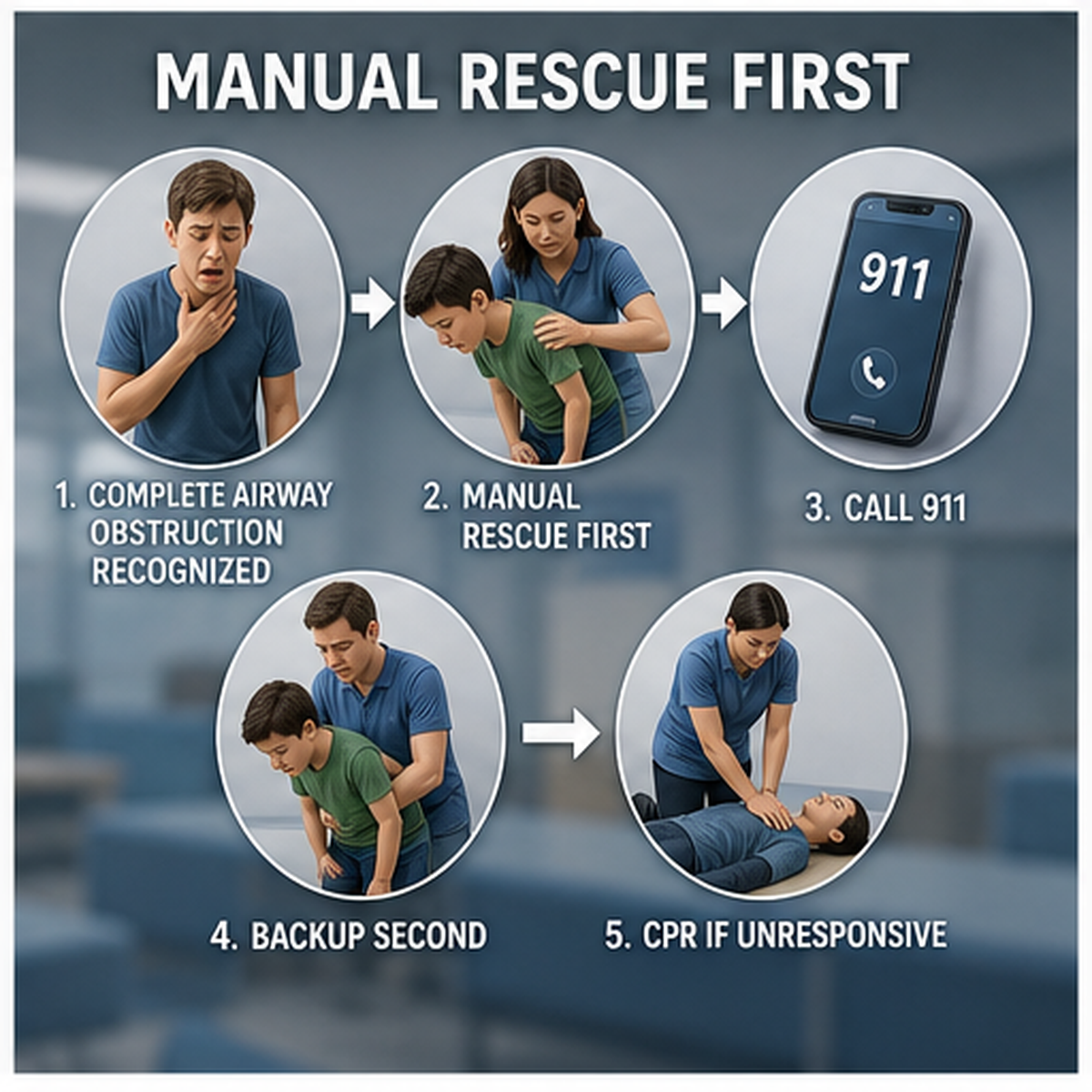
A useful school choking emergency plan has four moving parts: adults who recognize severe choking, a first-line response that starts immediately, clear 911 and nurse notification, and a second-line device placed where trained staff can reach it without abandoning the child.
For years, many school staff heard choking training reduced to a single phrase: do the Heimlich maneuver. That language is still familiar, but it is too narrow for current school training.
The 2025 American Heart Association update says conscious children and adults with severe choking should receive alternating cycles of 5 back blows followed by 5 abdominal thrusts until the object is expelled or the person becomes unresponsive. For infants, the sequence is 5 back blows followed by 5 chest thrusts, and abdominal thrusts are not recommended for infants.
That change matters in schools because lunch monitors, substitutes, coaches, bus staff, and after-school workers may not be medical professionals. They need a sequence they can remember under noise and pressure. The staff member closest to the child should not be wondering whether the first move is a phone call, a nurse search, a device search, or abdominal thrusts only.
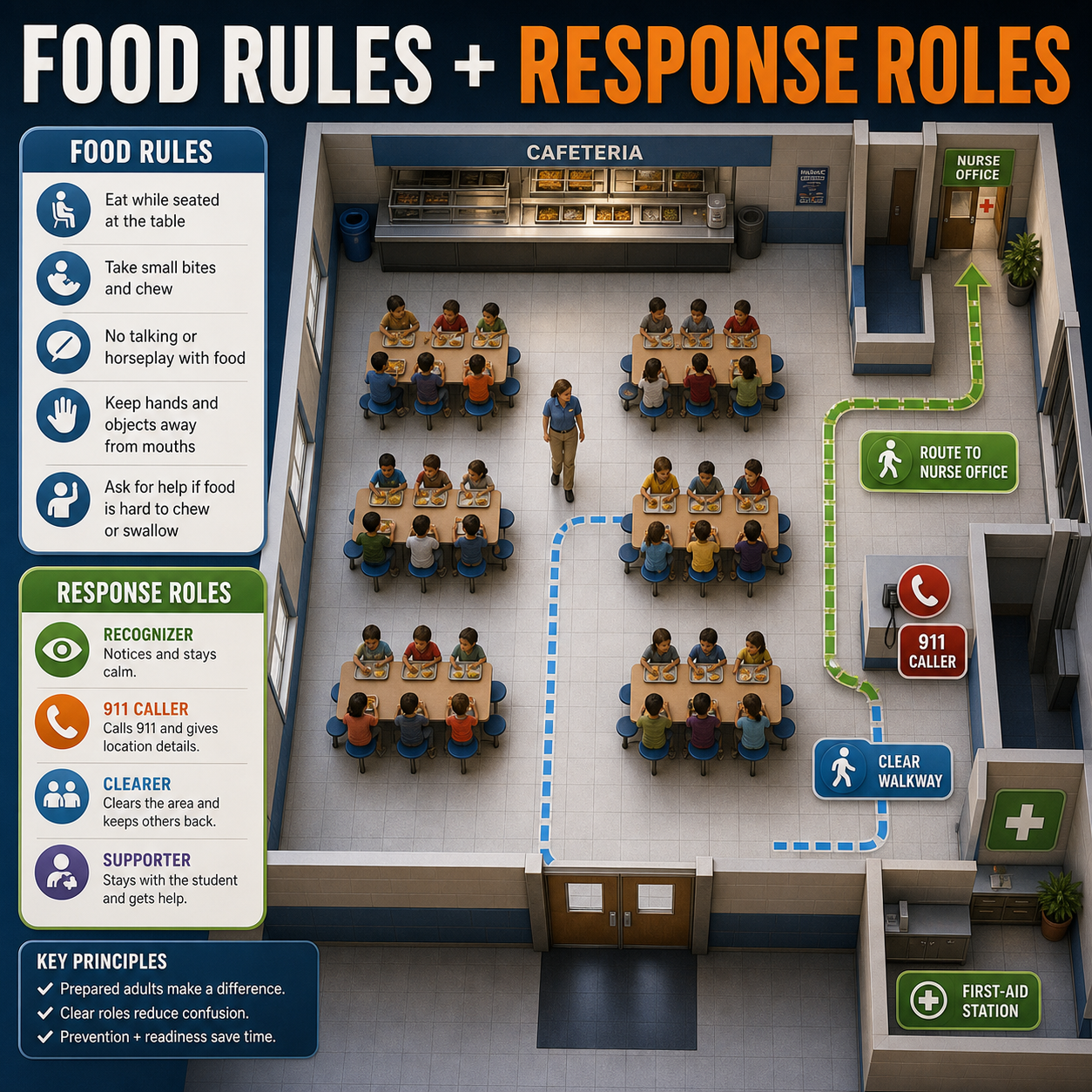
In a school choking first aid kit or cafeteria safety plan, the first sentence should be plain: if a responsive student over age 1 cannot cough, speak, or breathe effectively, start 5 back blows and 5 abdominal thrusts while another adult calls 911.
School choking safety is no longer only a local purchasing preference. Texas House Bill 549, the Westyn Bryan Mandrell Act, applies beginning with the 2025-2026 school year. The enrolled bill defines an airway clearance device as a noninvasive device capable of removing or assisting with the removal of a person's foreign-body airway obstruction. It requires each public school district campus to make at least one airway clearance device available if the device can be obtained through donation, purchase, lease, or designated funding.
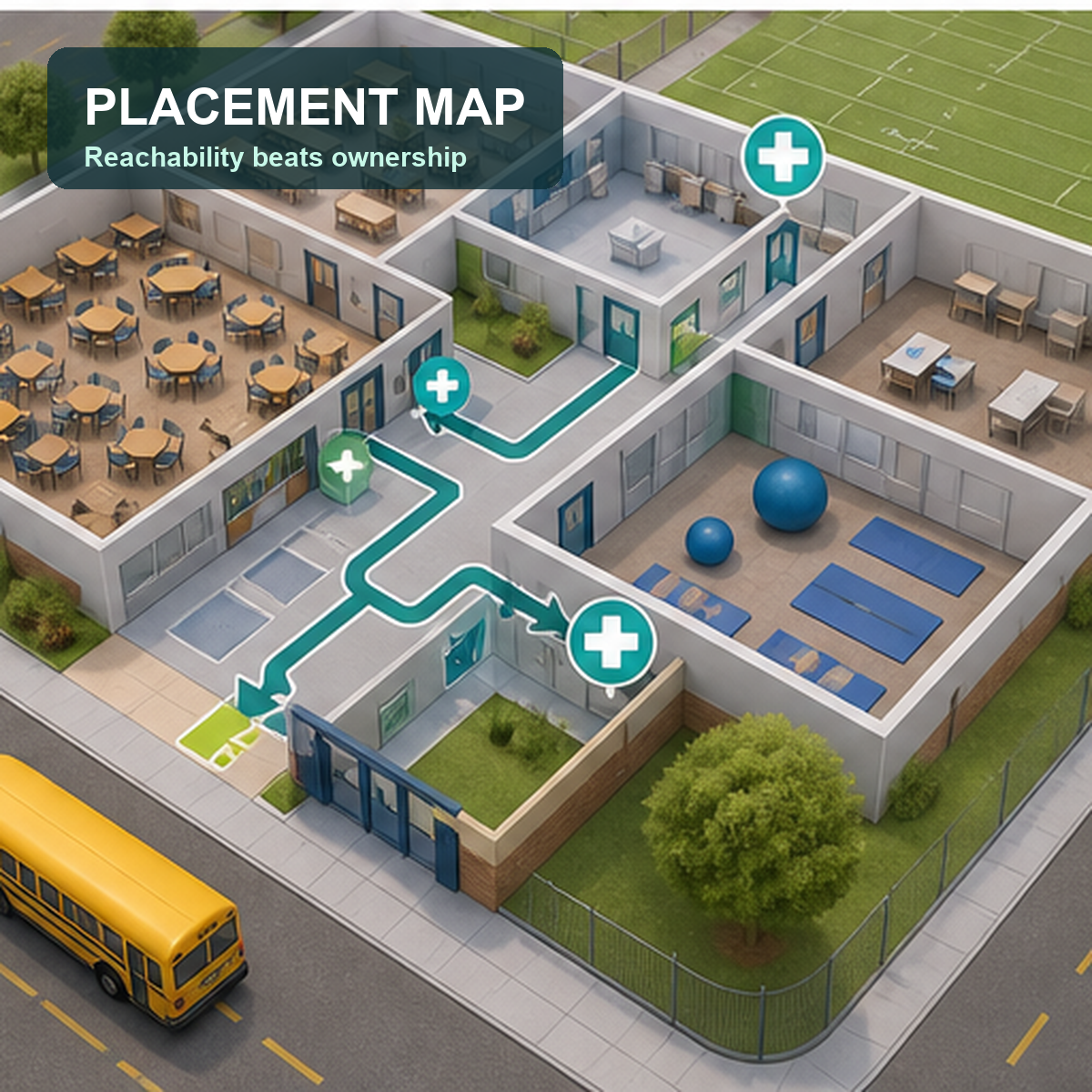
The most important language for deployment is not just the device requirement. It is the storage logic. The campus principal must consider the primary location where students consume food when deciding where to store the device. The bill also requires at least one trained campus or district employee to be present at each storage location whenever a substantial number of students are present there.
That is a placement rule, not a trophy rule. It pushes schools toward the cafeteria, snack areas, and other eating zones instead of treating the nurse's office as the automatic answer.
In March 2026, FDA's De Novo order for DEN250012 classified a suction anti-choking device under 21 CFR 874.5400, product code QXN. FDA identifies this device type as a suction anti-choking device as a second-line treatment. The order describes use for complete airway obstruction after unsuccessful use of a basic life support choking protocol.
That boundary is useful for schools because it prevents device-first thinking. A school choking rescue device should not be written into policy as the first thing staff reach for. First-line choking care begins with recognition, 911 delegation, and age-correct manual response. A QXN device may enter the response only as backup after those steps fail, if district policy permits it and trained staff can access it without delaying care.
A safer school policy does not say, 'We bought a device, so we are covered.' It says where the device is stored, who is trained, when it is retrieved, what manual steps must continue, and how EMS is handed the incident when they arrive.
A single storage location rarely fits a real campus. Students eat in cafeterias, classrooms, hallways during events, outdoor concession areas, gyms, buses, and after-school programs. A nurse's office may be important for inventory, extra masks, documentation forms, and staff training materials, but it should not be the only answer if meal activity happens elsewhere.
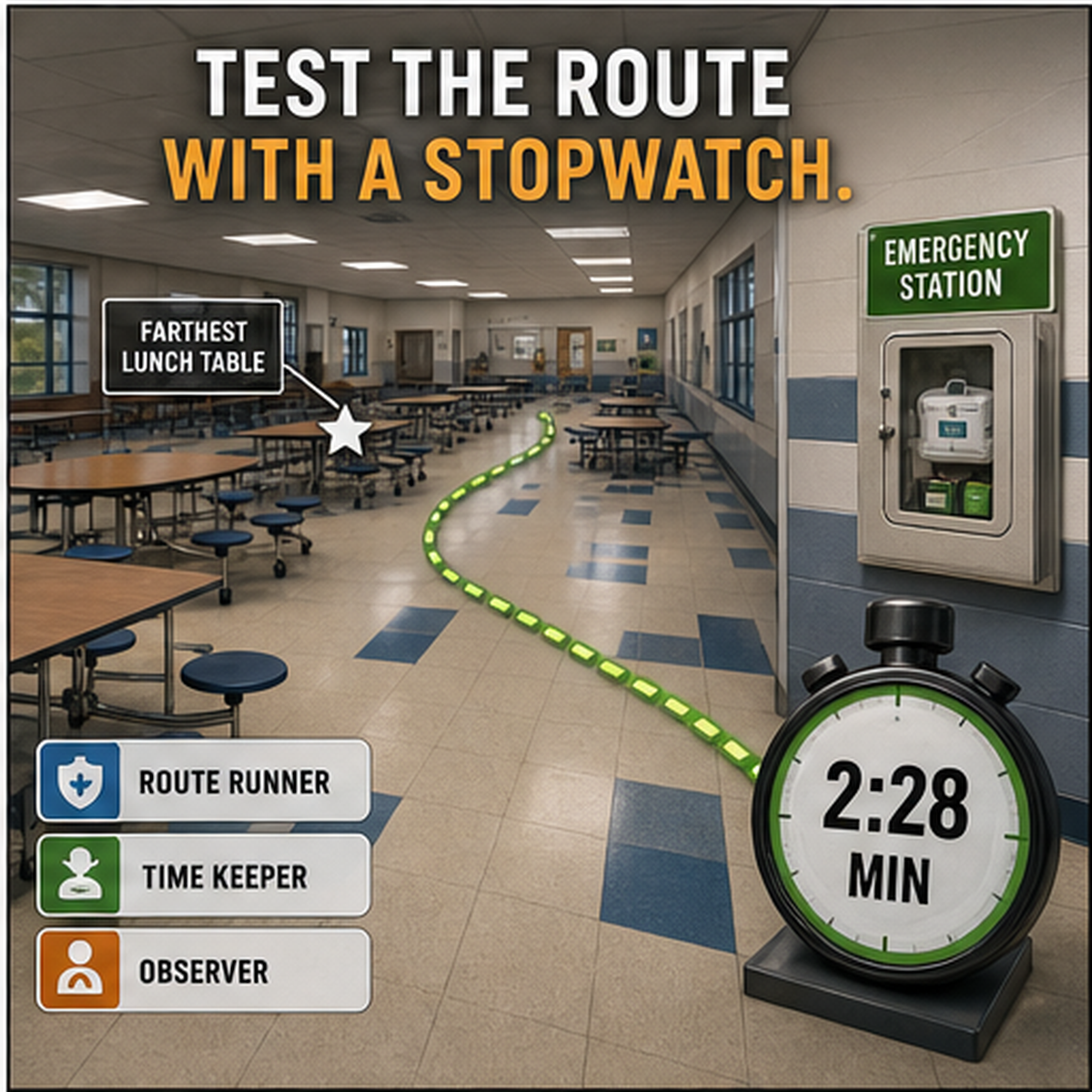
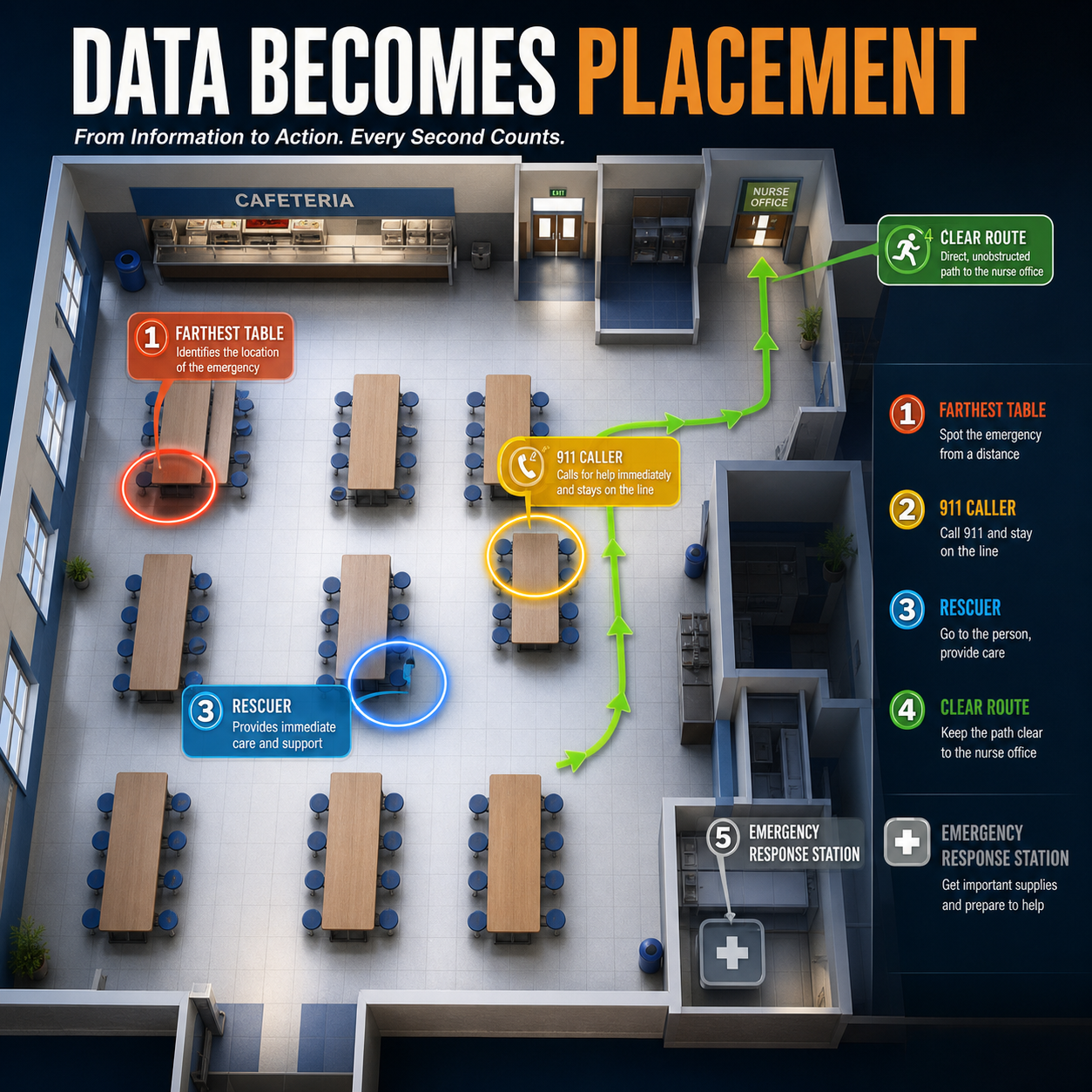
The most practical way to plan placement is to walk the campus during actual meal movement. Stand at the far lunch table. Walk to the proposed device location. Count doors, turns, locked areas, student crowding, and adult coverage. Then ask whether the only rescuer would have to leave the choking student to retrieve the device.
If the answer is yes, the school has a retrieval problem, not just an equipment problem.

Recommended next step
Map the cafeteria first. Then choose a Fitiger backup option that can be staged where trained staff can reach it without delaying manual first aid.
School buyers usually ask about price, brand, regulatory status, and whether the device comes with a wall case. Those are fair questions, but they are not enough. The sharper questions are operational.
Will cafeteria staff know when not to use it? Will substitutes know where it is? Can it be reached during after-school care when the nurse has left? Does the device fit the age range of the students? Does the policy say manual first aid comes first? Will staff practice opening the case, selecting the correct mask, creating a seal, and returning to CPR if the child becomes unresponsive?
A portable airway rescue device can look simple in a product photo. A real cafeteria is louder, messier, and less forgiving. Buying decisions should be made for that room, not for a brochure.
A school that takes choking preparedness seriously does not build one universal rule for every hallway. It builds a campus map.
Campus zone | Risk variable | Practical deployment standard | What to avoid |
|---|---|---|---|
Cafeteria | Highest meal density, noise, and distraction | Device station and trained staff within fast reach of lunch tables and serving line | Storing the only device in a distant nurse office |
Nurse office | Clinical support, documentation, spare supplies | Inventory base, staff reference point, and post-incident follow-up area | Treating the nurse office as the only response location |
Classroom snack areas | Food appears outside the cafeteria | Clear role plan and nearby phone access for teachers and aides | Assuming cafeteria policy covers classroom food |
Special education rooms | Communication limits, feeding support, individualized risk | Student-specific response radius and staff training | Using one generic cafeteria-only plan |
Athletic fields and after-school zones | Distance from main office and lower staffing | Portable emergency kit and EMS entrance plan | Forgetting concessions, team snacks, and after-hours events |
Bus loop and travel programs | Crowding, movement, poor line of sight | Staff call path and clear EMS handoff location | Depending on a device inside the locked main building |
Schools do not need every cafeteria monitor to become a clinician. They do need enough role practice that the first minute is not improvised. A 10-minute drill can do useful work if it is repeated and specific.
Start with recognition: can the student cough or speak? Then assign roles: rescuer, 911 caller, nurse or office runner, EMS entrance guide, and student crowd manager. Walk the actual path from the lunch table to the device station. Practice clear words: 'You call 911.' 'You get the nurse.' 'You meet EMS at Door 2.'
The device portion of the drill should be honest. Staff should know that an FDA-authorized choking rescue device is not a replacement for back blows and abdominal thrusts. It is a documented backup after unsuccessful manual care. If the school cannot explain that in one sentence, the training is not ready yet.
Many choking plans are written for the cafeteria at noon. Schools are bigger than that.
Special education classrooms may include students with feeding support needs, developmental differences, seizure history, dysphagia risk, or communication limitations. A student may not signal distress in the way staff expect. After-school programs may run with fewer adults and different access to the nurse's office. Athletic fields and concession stands may be far from the main building. Bus areas can be crowded, loud, and hard for EMS to access quickly.
A serious choking preparedness plan should mark those zones on the map. The question is not whether they appear in the master policy. The question is whether the closest adult has a job, a phone path, and access to the right support.
The most common failure is not refusing to buy equipment. It is buying equipment and then treating ownership as readiness.
A wall-mounted choking emergency device may reassure parents during a tour. A district inventory spreadsheet may reassure administrators. Neither one clears an airway if the device is behind the wrong door, staff do not understand second-line status, or nobody has rehearsed the first 60 seconds.
School choking safety equipment has to be treated like a response tool, not a display item. The same is true for a choking emergency kit, AED, or first aid station. Placement, training, access, documentation, and role assignment decide whether the tool is useful when the room gets quiet.
Walk the cafeteria before lunch. Stand where the quietest student would sit. Look for the nearest trained adult, the closest phone, the nurse route, the EMS entrance, and the device station. If any part of the answer depends on luck, memory, or a locked office, the plan is not finished.
A school choking emergency plan should make the first minute less chaotic. Manual first-line care starts the rescue. 911 gets delegated. The nurse and EMS route are clear. If an FDA-authorized QXN suction device is part of the campus plan, it sits in a reachable backup position after unsuccessful BLS choking protocol, not as a shortcut around training.
That is the difference between owning school choking safety equipment and building readiness around it.
Map every location where students eat, including cafeterias, classrooms, buses, events, and after-school programs.
Confirm the current first-line choking response sequence for staff training: 5 back blows + 5 abdominal thrusts for responsive students over age 1.
Define who calls 911, who starts care, who gets the nurse, who moves students back, and who meets EMS.
Place any choking rescue device or airway clearance device where trained staff can reach it quickly.
Write the second-line device rule plainly: use only after unsuccessful BLS choking protocol and only according to labeling and school policy.
Run short drills during real lunch-area conditions, not only in quiet staff meetings.
Review special education, sports, field trip, and after-school coverage separately.
Document training, device location, replacement schedule, and post-incident review steps.
Build the school choking plan before the lunchroom gets loud.
Explore Fitiger school airway readiness resources, placement planning, and second-line choking-readiness options for trained staff after standard manual choking first aid fails.
Make placement easier before lunch starts
Choose the response location before the purchase order closes. A device belongs in a reachable plan, not only an inventory list.
For related planning context, review the anti-choking device buyer evidence checklist.
There is no single national rule requiring every U.S. school to have an anti choking device. Some states are moving faster. Texas HB 549 applies beginning with the 2025-2026 school year and requires eligible public school campuses to make at least one airway clearance device available when obtained through donation, purchase, lease, or designated funding. Schools should also check state law, district policy, and local legal guidance.
Place it where students actually eat and where trained staff can reach it quickly. Cafeterias, snack areas, special education meal spaces, and after-school food zones may be more useful than a locked office. Texas HB 549 specifically says campus principals must consider the primary location where students consume food when storing the device.
No. For conscious children and adults, current AHA guidance uses 5 back blows followed by 5 abdominal thrusts. FDA's QXN category places suction anti-choking devices as second-line treatment after unsuccessful BLS choking protocol, not as a replacement for manual first aid, 911, EMS, or CPR.
If the student can cough forcefully, encourage coughing and stay close. If the student cannot cough, speak, cry, or breathe effectively, begin age-correct choking first aid and delegate 911. For a responsive student over age 1, that means repeated cycles of 5 back blows and 5 abdominal thrusts.
Usually not. The nurse's office can hold extra supplies and records, but a device stored far from the cafeteria or snack area may not help in the first minute. Schools should map retrieval time from the places where choking is most likely to be noticed.
At minimum, staff stationed near the device location should be trained. Cafeteria monitors, school nurses, front office staff, coaches, special education staff, after-school staff, and substitutes may all need role-specific instruction depending on where students eat and gather.
No. The FDA QXN category is for complete airway obstruction after unsuccessful BLS choking protocol. Device labeling, student age, mask fit, school policy, staff training, and emergency status all matter. It should not be used for mild choking or a student who can cough forcefully.
A useful drill should include recognition of severe choking, 911 delegation, first-line manual response, nurse or office notification, EMS entrance guidance, device retrieval, and the transition to CPR if the student becomes unresponsive.
Ask about FDA authorization, age range, instructions for use, training materials, wall placement options, replacement parts, documentation support, and whether staff can realistically retrieve and use the device without delaying first-line care.
The best cafeteria plan is role-based and location-specific: one adult starts care, one calls 911, one clears students back, one guides the nurse or EMS, and any second-line device is staged close enough to be reached without leaving the student unsupported.
American Heart Association - 2025 CPR and ECC Guidelines newsroom summary. Supports the updated choking sequence: 5 back blows + 5 abdominal thrusts for conscious children and adults, and 5 back blows + 5 chest thrusts for infants.
FDA De Novo DEN250012. - 21 CFR 874.5400, product code QXN, and the suction anti-choking device as a second-line treatment after unsuccessful BLS choking protocol.
Texas HB 549, Westyn Bryan Mandrell Act. - state-level school airway clearance device availability, storage-location logic, and trained-employee presence requirements beginning with the 2025-2026 school year.
American Red Cross - Choking first aid. Supports public-facing recognition and response training.
HealthyChildren.org / American Academy of Pediatrics. - child choking prevention, food-risk education, and school/family safety education.
This article is for general education and emergency preparedness only. It does not replace professional medical advice, certified CPR or first-aid training, emergency medical services, school district policy, legal advice, or device instructions for use. In a choking emergency, call 911 or your local emergency number and follow dispatcher instructions.




















