A damaged package does not automatically prove device failure. It removes the safety of assumptions. If a seal is broken, a pouch is opened, or a box is crushed enough to raise doubt, the unit no longer sits in the original controlled storage state that supported emergency readiness.
For a household checklist, see Fitiger's child and home choking safety readiness plan.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.

A clean box gives people confidence. A sealed pouch gives even more. In a home kitchen drawer, a school cafeteria cabinet, a restaurant emergency station, a nursing-home dining room, or a vehicle emergency kit, packaging is often the first sign that an emergency airway device has been protected from handling, dust, moisture, and missing-part drift.
Once the package is damaged, the question changes. It is no longer only, "Do we own a choking rescue device?" The harder question is, "Can we still trust this exact unit as staged-ready backup?"
Emergency airway device packaging damage matters because the device is supposed to serve as a backup layer after first-line rescue has not cleared the airway. A backup layer should not arrive with unanswered questions about barrier integrity, missing parts, storage condition, or access friction.
A broken seal does not prove the device will fail. It proves blind trust is no longer justified.
People often separate the product from the package. That works for ordinary consumer goods. It is weaker thinking for emergency equipment.
The package protects the device during storage. It keeps instructions with the unit. It keeps masks, connectors, and accessories from drifting into another drawer or bag. It reduces uncertainty about whether the device has been handled, exposed, or partly assembled by someone trying to "check it quickly" before putting it back.
For a suction anti-choking device, packaging also affects time. FDA has warned that removing, unpacking, and assembling an anti-choking device may delay care. That warning cuts both directions: unopened packaging can slow access if staff have never practiced; opened packaging can create uncertainty if parts shift or instructions separate.
A readiness plan has to control both problems: protection before use and speed during use.
Packaging condition does not change the rescue sequence.
Established choking rescue protocols come first. 911 or local emergency services should be activated early. CPR begins if the person becomes unresponsive. Under FDA 21 CFR 874.5400 and product code QXN, a suction anti-choking device is a second-line treatment after unsuccessful use of a basic life support choking protocol for complete airway obstruction.
A perfect package does not move the device earlier. A damaged package does not make the device more urgent. The device remains backup, and the manual-first sequence remains the safety foundation.
Complete airway obstruction means the person cannot move enough air to breathe, speak, cry, or cough effectively. Forceful coughing usually means air is still moving and should not be treated the same way as complete obstruction.
This distinction matters when emergency equipment is visible on a wall or inside a kit. A responder may see panic and reach for the device too early. Packaging damage can make that moment worse because the responder now has to decide whether the unit is usable while the person may still be coughing forcefully. Training should keep the threshold clear: standard choking first aid first, and any suction anti-choking device only within its labeled second-line role.

A broken seal is not a diagnosis. It is a change in evidence.
Once the seal is broken, the site can no longer assume the unit remains inside the same protected storage state. Moisture exposure, dust exposure, handling history, missing instructions, shifted masks, contamination risk, and access behavior all become open questions.
For an anti choking device for home, this may happen when a parent opens the pouch to see what is inside and then drops it back into the drawer. For school choking safety equipment, it may happen when a staff member opens the kit during a drill but does not document restaging. For a restaurant choking emergency station, it may happen when a manager checks the unit, separates the instructions, and puts the package back loosely.
The correct response is not panic. The correct response is inspection, documentation, and a clear restage or replacement decision.

A crushed outer carton is not automatically the same as a punctured primary pouch. Some box damage is cosmetic. Some is not.
The right question is whether the force reached the protected contents. Did the inner pouch crease, split, puncture, or open? Did the seal line deform? Did the instructions tear or separate? Did a mask become compressed, warped, or displaced? Did a connector shift? Did the box damage make the device harder to access under stress?
A vehicle emergency kit makes this especially easy to miss. A trunk organizer can crush the box under other supplies. A family may see the carton later and decide it is just cardboard. But if the inner barrier or mask shape changed, the staged condition changed too.
A crushed box should trigger inspection before the unit remains in routine emergency staging.
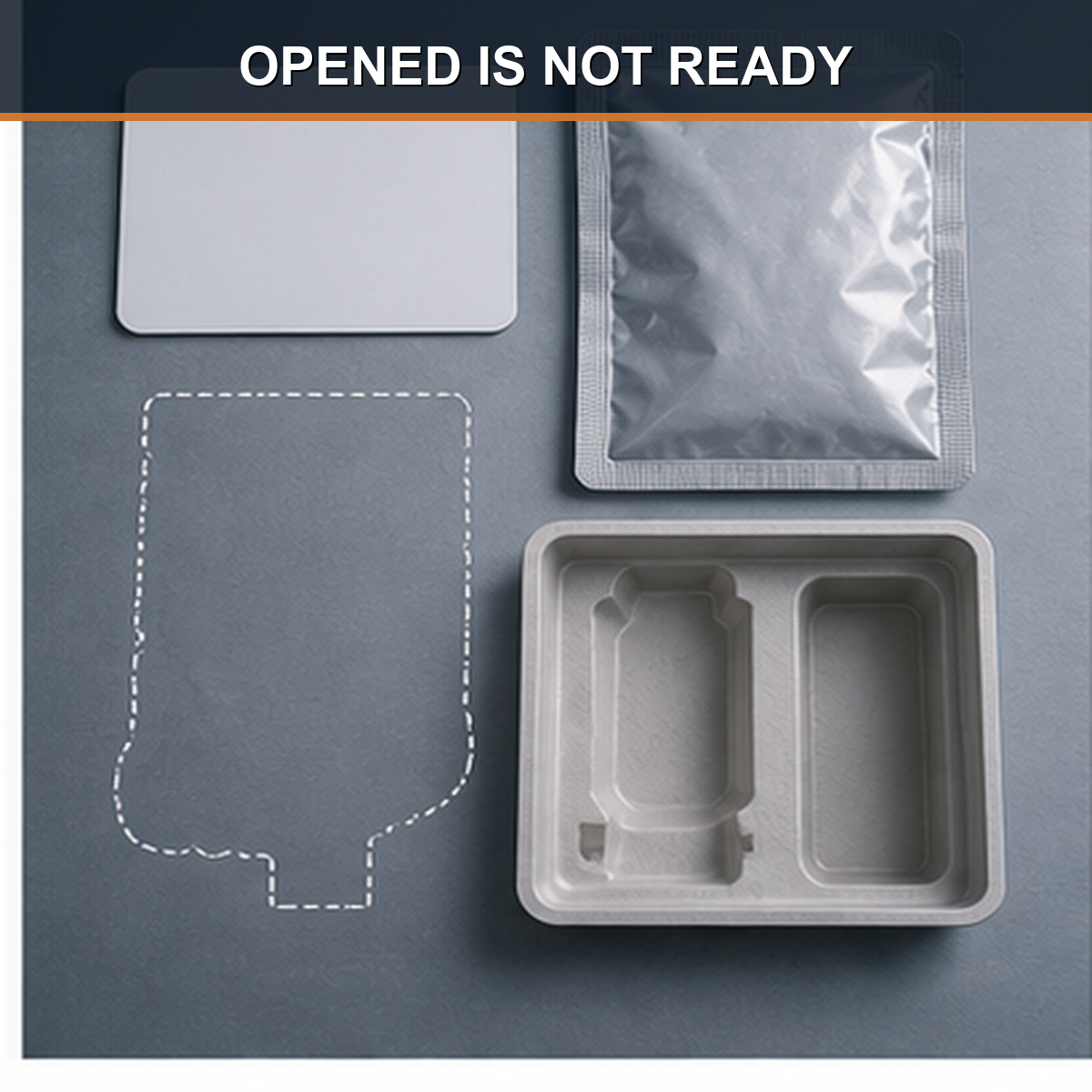
Opened pouches create a practical trap.
Someone opens the pouch "just to check it." The device becomes easier to see. That can feel like faster access. But the same action may separate instructions, loosen parts, expose the unit to dust or moisture, or leave masks unsecured. The kit may become less protected and less predictable at the same time.
For a choking emergency kit in a school cafeteria, this can turn into a drill failure months later. A staff member opens the cabinet, sees the device, and then has to search for the right mask, the instruction card, or a missing accessory. The package was open, but the system was not faster.
A pouch opened for convenience needs a documented restaging decision. Otherwise, the kit has moved from controlled readiness into habit-based trust.
|
Condition |
Operational Meaning |
Readiness Judgment |
|---|---|---|
|
Intact sealed primary pouch |
Closest to original staged condition |
Highest confidence, subject to normal shelf-life and scheduled inspection |
|
Outer box dented, inner pouch intact |
Impact history now matters |
Inspect the inner pouch, instructions, masks, and access path before continued staging |
|
Inner pouch creased, punctured, split, or partly opened |
Original protected state can no longer be assumed |
Remove from blind-trust staging until evaluated or replaced |
|
Seal broken, contents loose, or parts separated |
Storage certainty and access certainty both degraded |
Highest concern; replace, restage formally, or remove from emergency station |
|
Opened for convenience and returned to kit |
May reduce one delay while creating missing-part or barrier uncertainty |
Audit parts, instructions, cleanliness, seal state, and access friction |
|
Vehicle kit with crushed or heat-stressed packaging |
Unknown thermal and mechanical history |
Inspect packaging, mask shape, seals, instructions, and expiration; consider indoor replacement stock |
A damaged package inspection should be simple enough for a family, school, restaurant, or care facility to perform consistently. It should answer three questions.
First: is the protective barrier still intact? Second: are all parts present, identifiable, clean, and stored together? Third: can a responder access and use the kit without adding confusion to the manual-first sequence?
If the answer to any of those questions is uncertain, the unit should not remain in blind-trust staging.
|
Inspection Point |
What to Check |
Why It Matters |
|---|---|---|
|
Outer package |
Crushing, tears, water stains, heat marks, label damage |
Shows whether the kit has had mechanical or environmental stress |
|
Primary pouch or seal |
Puncture, split, opened edge, broken seal, loose contents |
Determines whether protected storage can still be assumed |
|
Device body |
Cracks, deformation, discoloration, tackiness, unusual odor |
May indicate storage stress or material drift |
|
Mask condition |
Warping, compression, dirt, missing size, poor flexibility |
Mask condition affects face seal and user confidence |
|
Valve or connector area |
Visible debris, deformation, loose fit, shifted parts |
Seal paths and airflow control depend on component integrity |
|
Instructions for use |
Present, readable, stored with device |
Instructions help prevent device-first or wrong-use behavior |
|
Expiration / shelf-life |
Date, storage conditions, replacement schedule |
Shelf-life depends on defined storage assumptions |
|
Access friction |
Locks, packaging difficulty, missing scissors, blocked route |
Time lost to access friction can weaken second-line readiness |
|
Inspection record |
Date, inspector, deficiency, action taken |
Readiness needs ownership, not memory |
Packaging damage is not the same in every environment. A home drawer, school cafeteria, restaurant station, nursing-home dining room, vehicle trunk, and community event kit all create different failure modes.
|
Setting |
Common Packaging Risk |
Best Readiness Action |
|---|---|---|
|
Home kitchen or hallway |
Family opens pouch to inspect, then returns loose parts |
Use a simple monthly check; replace or restage if seal or instructions are no longer controlled |
|
School cafeteria |
Kit opened during drill, moved, or stored behind other supplies |
Use QR check logs, room-level location, and a named inspection owner |
|
Special education classroom |
Frequent staff access and high activity around storage area |
Keep kit visible, protected, and tied to a manual-first response role card |
|
Nursing-home dining room |
Moisture, cleaning supplies, tray traffic, or cabinet crowding |
Inspect barrier condition and access path during dining-room readiness rounds |
|
Restaurant emergency station |
Box crushed behind supplies or instructions separated |
Assign manager inspection and keep emergency station uncluttered |
|
Vehicle emergency kit |
Heat cycling, crushing, and long idle time |
Check heat history, seal condition, expiration, and mask shape more often |
|
Church or community event kit |
Set up and taken down repeatedly by volunteers |
Use a setup checklist and verify the kit before food service begins |
Schools are especially vulnerable to the inventory illusion. The device exists, but the exact readiness condition is unclear.
A school may have a choking rescue device for schools in the nurse office, cafeteria, or athletic area. If the pouch is open, the seal is broken, or the box is crushed, staff should not rely on memory. A QR check log or inspection record should show the last verified condition, who checked it, what deficiency was found, and whether the device was replaced, restaged, or removed.
For school choking safety equipment, the strongest record is room-specific. It should not only say the school owns the device. It should show that the cafeteria station, nurse-office unit, SPED classroom kit, or athletic-area kit passed its last check.

A vehicle emergency kit lives a harder life than an indoor cabinet.
Heat, cold, vibration, trunk compression, grocery loads, sports equipment, and long idle time all push on packaging and materials. A portable choking rescue device stored in a car may be useful for family travel, school pickup, sports practice, and rural driving, but storage discipline has to match the environment.
If the box is crushed or the pouch looks stressed after months in a vehicle, do not treat the kit as automatically ready just because the device has not been used. Heat exposure and packaging damage should be checked together.
Buyer concern: can I still use it if only the box is damaged?
Maybe. But the decision should not be based on the outer box alone.
If the outer carton is dented but the inner pouch is sealed, dry, unpunctured, and the device, mask, instructions, and accessories are undisturbed, the unit may still be suitable for continued staging according to the manufacturer's instructions and facility policy. If the inner pouch is creased, torn, opened, moist, or partly separated, the confidence level changes.
The safest operational rule is simple: outer damage triggers inspection; primary barrier damage triggers removal from blind-trust staging.
Buyer concern: should I replace it if the pouch is open?
An opened pouch does not automatically prove the device is unusable. It does mean the original sealed storage state is gone.
For a family kit, replacement may be the cleanest choice if the device is intended for emergency readiness and the barrier state is now uncertain. For a school, care facility, restaurant, or public venue, an opened pouch should trigger the site's inspection and restaging process. If the kit cannot be verified, it should not remain the unit people depend on in the next emergency.
Buyer concern: does a broken seal mean contamination?
Not always. A broken seal means contamination cannot be ruled out with the same confidence. It also raises questions about moisture, dust, handling, missing parts, and whether the device was stored according to the assumptions behind its readiness state.
Contamination is only one part of the decision. Access predictability and completeness matter too. A clean-looking opened pouch can still be a poor emergency station if the instructions are missing or parts have shifted.
|
Situation |
Do Not Assume |
Practical Action |
|---|---|---|
|
Outer carton slightly dented, primary pouch intact |
Do not assume all damage is cosmetic |
Inspect pouch, contents, instructions, and access; document continued staging if acceptable |
|
Primary pouch open or punctured |
Do not assume the device is still protected |
Remove from blind-trust staging; replace or evaluate according to policy and IFU |
|
Instructions missing or separated |
Do not assume staff will remember use boundaries |
Restage with complete instructions or replace the kit |
|
Device loose in a drawer or box |
Do not assume parts are clean, complete, or fast to identify |
Rebuild controlled kit or replace with intact staged unit |
|
Vehicle-stored kit after heat and crushing |
Do not assume date alone proves readiness |
Check heat history, packaging, mask, seal, expiration, and device condition |
|
School kit opened after drill |
Do not assume the drill ended with correct restaging |
Run post-drill inventory, seal check, and QR status update |
A responsible article has to keep evidence boundaries clear.
Packaging damage can support concern. It can support inspection, restaging, replacement, or removal from routine emergency use. It cannot prove device failure by itself. It cannot prove suction performance has changed without appropriate evaluation. It cannot move a suction anti-choking device ahead of manual rescue. It cannot convert a visual judgment into a validated performance conclusion.
That discipline protects both safety and credibility. A damaged package is not a verdict. It is a stop sign for assumptions.
A broken seal, crushed box, or opened pouch is not automatically a failed device. It is a failed assumption.
The right response is inspection, documentation, and a clear decision before the next emergency. The wrong response is to put the unit back because it still looks mostly fine.
Manual choking rescue remains first. 911 happens early. A suction anti-choking device remains second-line backup after unsuccessful BLS choking rescue for complete airway obstruction.
Before the next school lunch, restaurant shift, nursing-home meal pass, family trip, or community event, check the package before the room has to trust it.
For related planning context, review the anti-choking device buyer evidence checklist.
No. A damaged package does not automatically prove device failure. It removes the safety of assumptions. The unit should be inspected, restaged, replaced, or removed from blind-trust staging until its condition is resolved.
A broken seal means the original protected storage condition can no longer be assumed. Barrier integrity, moisture exposure, contamination risk, handling history, missing parts, and access behavior all need review.
Not always. A crushed outer box is an inspection trigger. If the inner pouch and contents are intact, the unit may still be suitable for staging according to the manufacturer's instructions and facility policy. If the primary pouch or contents are affected, replacement or removal is safer.
Sometimes it may appear faster, but it can also create missing-part, contamination, instruction, and storage-certainty problems. An opened pouch should trigger a restaging decision, not casual trust.
No. Packaging condition does not change the rescue sequence. Established choking rescue protocols come first. A suction anti-choking device remains second-line after unsuccessful BLS choking protocol for complete airway obstruction.
Schools should inspect choking emergency kits on a scheduled basis and after any drill, relocation, cabinet change, suspected damage, or opened package. QR check logs can help show location, status, inspection date, and open deficiencies.
Vehicle storage needs stricter inspection because heat cycling, crushing, and long idle time can affect packaging and materials. Check the manufacturer's storage instructions, expiration, seal condition, mask shape, and package integrity before relying on a vehicle-stored kit.
Restaurants and community venues should check whether the kit is visible, sealed, complete, reachable from the food area, and not blocked by supplies. Staff should also know that manual rescue comes first and any device is second-line backup only.
Document the date, location, package condition, seal status, missing or shifted parts, action taken, replacement or restaging decision, and the person responsible for the check.
FDA Safety Communication, updated March 4, 2026 - Supports the manual-first sequence, public warning about device delay, and the position that established choking rescue protocols should come first.
FDA De Novo Order DEN250012 - Supports 21 CFR 874.5400, product code QXN, and the second-line treatment boundary for suction anti-choking devices after unsuccessful BLS choking protocol.
American Heart Association 2025 Choking Guidance - Supports the established first-line choking rescue sequence and CPR transition.
FDA Shelf Life of Medical Devices Guidance - Supports the principle that shelf-life is tied to acceptable specifications under defined storage conditions.
This article is for educational and preparedness planning purposes only. It is not medical advice, legal advice, first-aid certification, or a substitute for emergency medical services, professional clinical judgment, or product-specific instructions for use. In a choking emergency, call 911 or the appropriate local emergency number, follow current established choking rescue protocols, and use any device only within its labeled role and instructions.




















