Rural EMS systems now show total call times running nearly 20 minutes longer than the national average. Airway emergencies do not tolerate that gap. Once first-line BLS fails, readiness shifts to the people already on scene: trained responders, low-latency deployment, dispatcher guidance where available, and a lawful second-line backup layer that can be used inside the waiting window.
Coverage language still dominates too many rural safety conversations. More trucks. More stations. More mutual aid. Airway emergencies expose a different problem. The clock that matters is the gap between the start of obstruction and the first useful intervention on scene.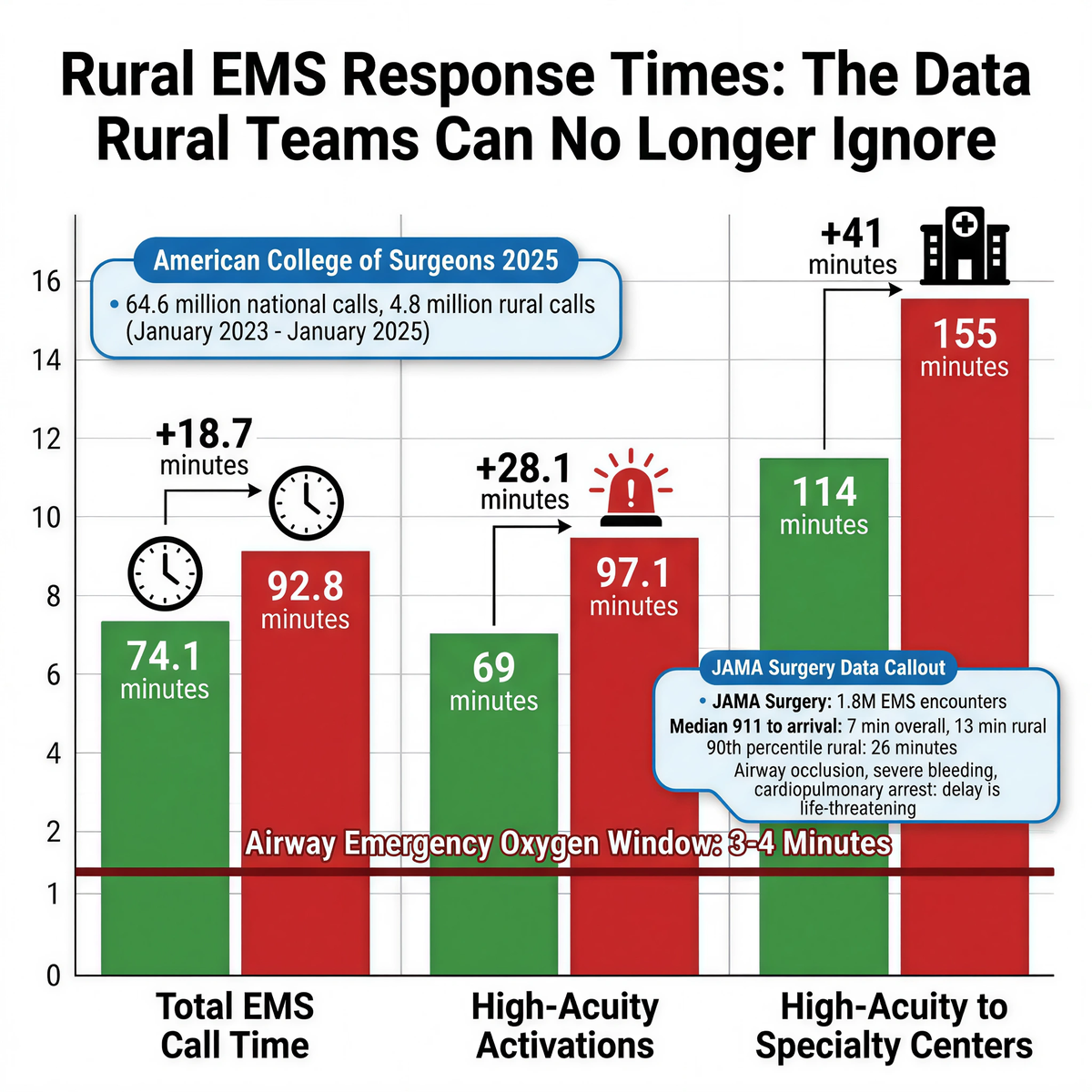
The American College of Surgeons reported in 2025 that, across National Emergency Medical Services Information System data covering 64.6 million national calls and more than 4.8 million rural calls from January 2023 through January 2025, total EMS call times in rural communities averaged 92.8 minutes compared with 74.1 minutes nationally. High-acuity rural activations averaged 97.1 minutes compared with 69 minutes nationally. For high-acuity patients transported to specialty centers, rural total call times reached 155 minutes compared with 114 minutes nationally.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
Those numbers are not airway-specific. They still define the environment the airway event happens inside. Longer response chains. Longer scene times. Longer transport intervals. Longer handoff paths. The emergency happens in that system, not in an urban benchmark.
Some emergencies tolerate delay better than others. Complete airway obstruction does not.
The JAMA Surgery analysis of nearly 1.8 million EMS encounters found a median time from 911 call receipt to first-unit arrival of 7 minutes overall, 13 minutes in rural zip codes, and a 90th percentile of 26 minutes in rural settings. The authors singled out airway occlusion, severe bleeding, and cardiopulmonary arrest as conditions where even modest delay can be life threatening.
A rural route can function normally for ten other incidents and still fail a choking event. Oxygen loss does not wait for dispatch efficiency, county lines, or highway distance to become convenient.
The planning mistake is easy to spot. A team writes a severe-airway protocol as if outside EMS is the next step after first-line BLS. In many non-urban zip codes, that assumption is false. The next step is still on scene.
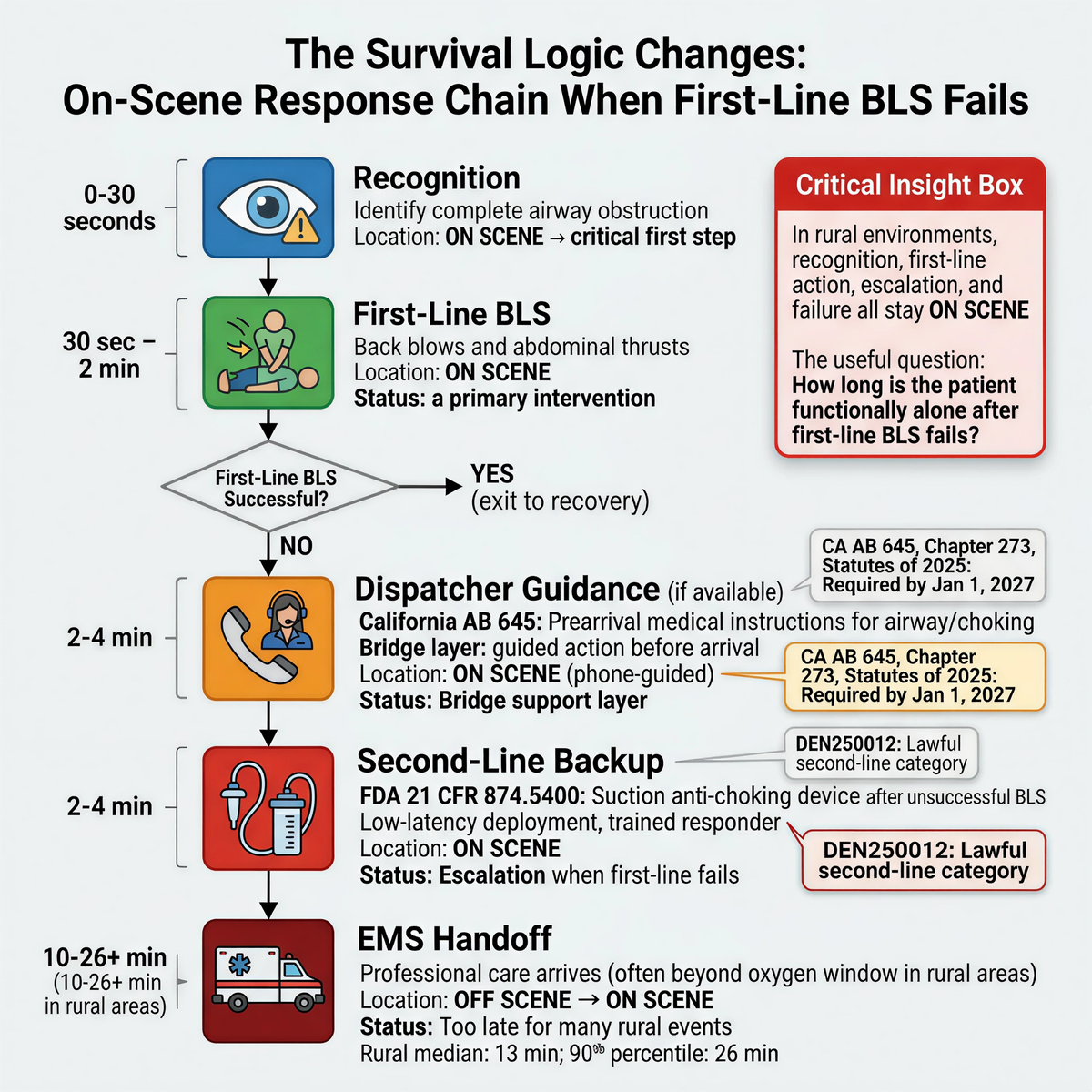
The shift is operational, not rhetorical. Recognition stays on scene. First-line manual response stays on scene. Escalation stays on scene. Failure stays on scene too. The useful question is no longer whether a hospital exists somewhere in the county. The useful question is how long the worker, rider, or student is functionally alone after first-line BLS has failed.
California's AB 645, Chapter 273, Statutes of 2025, requires public safety agencies that process 911 calls for emergency medical response to provide prearrival medical instructions by January 1, 2027, including airway and choking instructions for infants, children, and adults. The instructions must be approved by the local EMS agency medical director and implemented under local medical protocols.
That law matters far beyond California's borders because it names the bridge layer directly. Rural and non-urban systems do not close long arrival windows with optimism. They close them with guided action before arrival. Dispatcher coaching does not replace first-line rescue. It strengthens the chain between recognition and professional handoff. In a long-response environment, that chain becomes part of the system rather than a courtesy on the phone.
Federal authorization under DEN250012 created 21 CFR 874.5400 for a suction anti-choking device as a second-line treatment after unsuccessful use of a basic life support choking protocol. That gave procurement teams a lawful category. It also raised the engineering bar.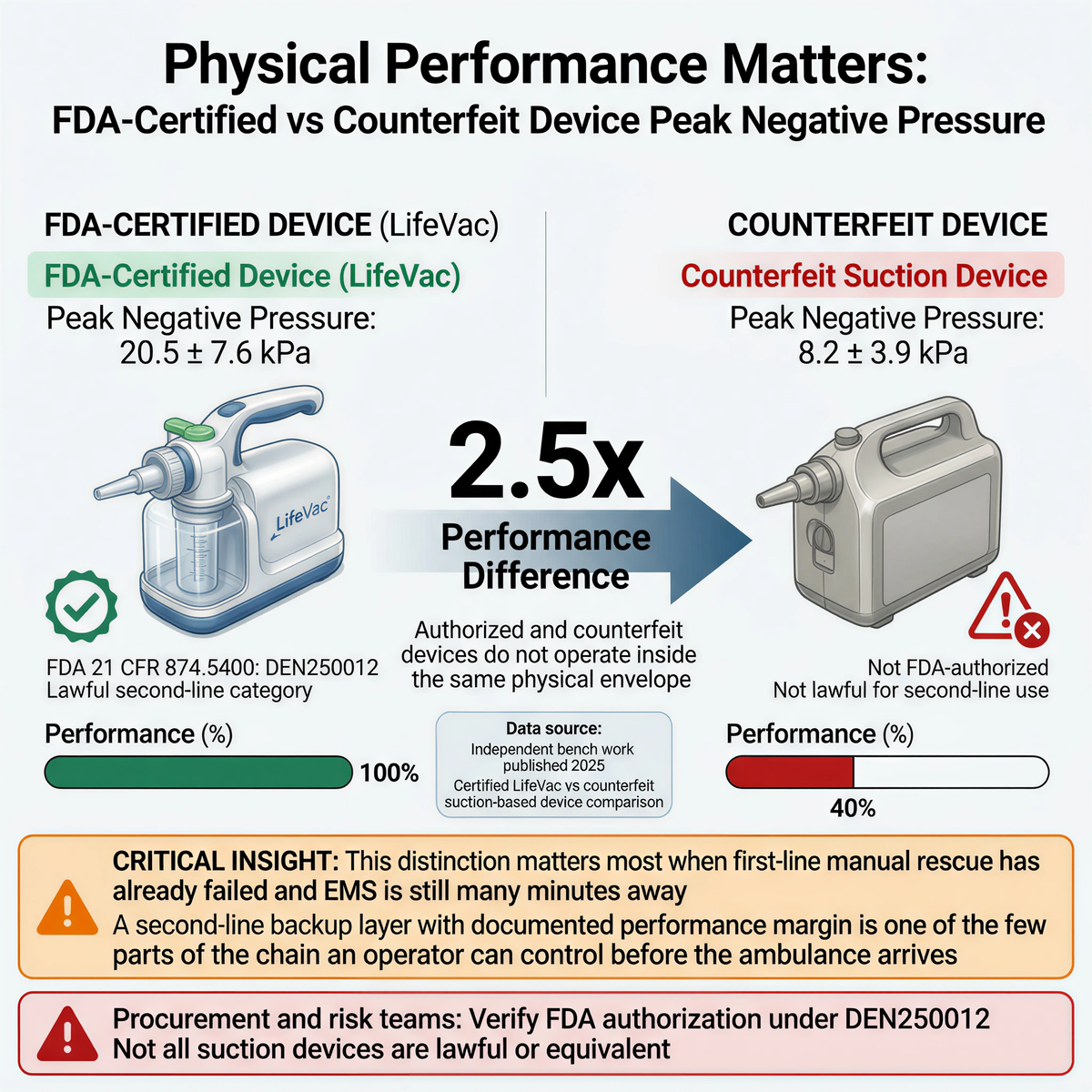
Independent bench work published in 2025 compared a certified LifeVac device with a counterfeit suction-based device and found peak negative pressure of 20.5 +/- 7.6 kPa for the certified device versus 8.2 +/- 3.9 kPa for the counterfeit device. That is roughly a 2.5x performance difference. Procurement and risk teams should read that carefully. This is not proof of clinical success by itself. It is proof that authorized and counterfeit devices do not operate inside the same physical envelope.
That distinction matters most when first-line manual rescue has already failed and EMS is still many minutes away. A second-line backup layer with a documented performance margin is not the whole rescue chain. In remote environments, it is one of the few parts of the chain an operator can control before the ambulance arrives.
Remote events often collapse onto one adult. One driver. One yard lead. One transport aide. One ranch supervisor. One person listening to a dispatcher while trying to keep a scene from degrading.
A 2023 simulated trial involving untrained health science students found median completion time of 36.6 seconds with LifeVac versus 50.4 seconds with DeCHOKER in an adult foreign body airway obstruction scenario. The gap is not just a stopwatch detail. Rural and mobile response chains punish complexity. A second-line device that can be described quickly, handled under stress, and integrated into phone-guided escalation has a better chance of fitting the real environment.
Fitiger's engineering and product safety view stays consistent here. High-stress lone-responder events strip away elegant theory. Shorter sequences, clear masks, predictable grip paths, and low-debate deployment matter more than polished training language when the only instructions still arriving are coming through a phone speaker.
We read rural airway risk as a latency chain: recognition latency, first-line action latency, second-line retrieval latency, second-line application latency, and EMS handoff latency. Rural response stretches every link after the first. The links that can actually be shortened are the ones controlled on scene.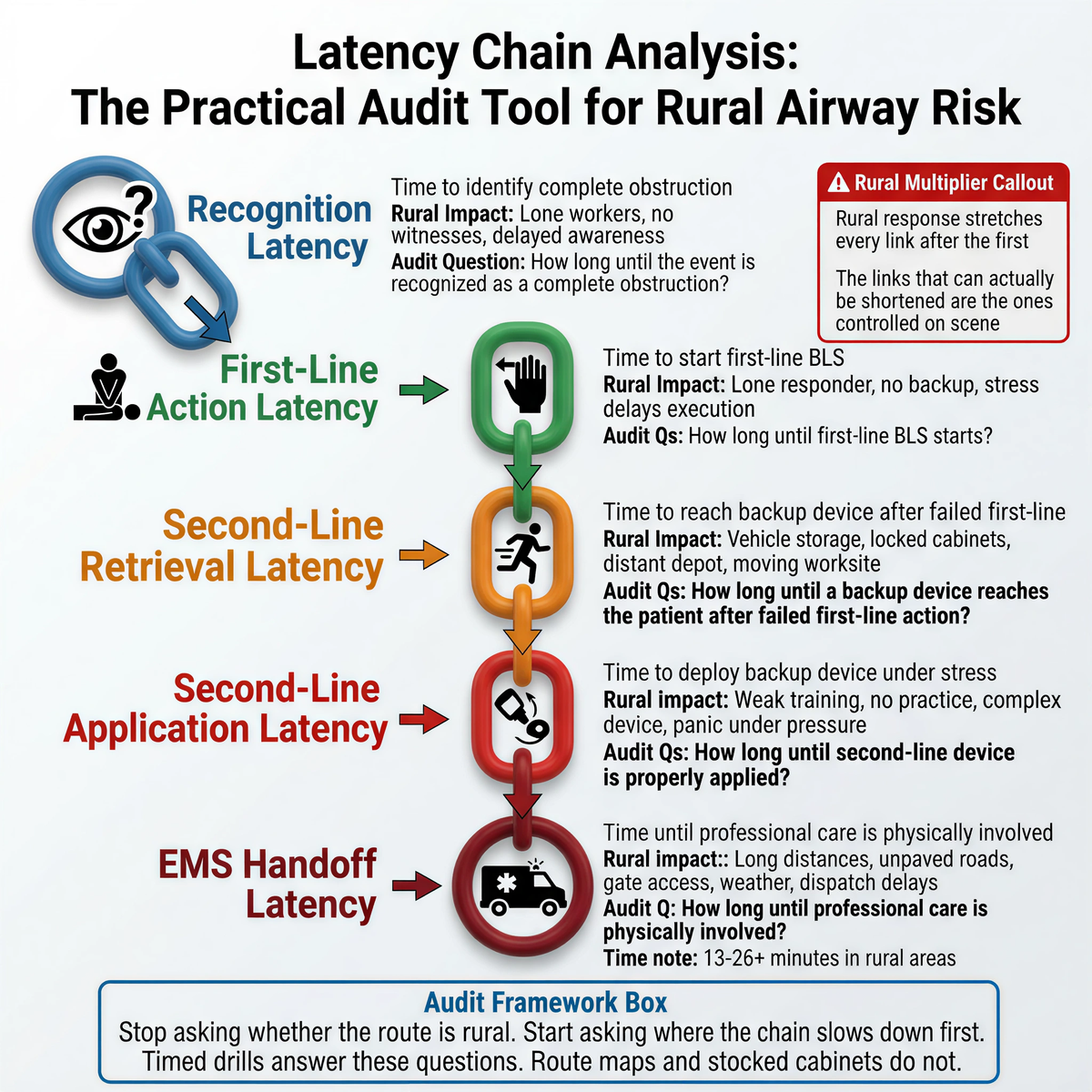
That framework changes the audit question. Stop asking whether the route is rural. Start asking where the chain slows down first.
- How long until the event is recognized as a complete obstruction?
- How long until first-line BLS starts?
- How long until a backup device reaches the patient after failed first-line action?
- How long until a dispatcher can support escalation, if that layer exists?
- How long until professional care is physically involved?
A route map, a clinic address, and a stocked cabinet do not answer those questions. Timed drills do.
Choose one remote depot, one vehicle route, or one outlying worksite this week.
Measure the path from the likely incident point to first-line action.
Measure the path from failed first-line action to second-line retrieval.
Write down the realistic first-unit arrival time, not the best-case estimate.
Check whether dispatcher-guided escalation is part of the local EMS environment.
Verify that any backup device in the plan is lawful under the current FDA framework, not merely listed for sale.
A team that has not timed the chain is still guessing.
Before you buy another unit or expand another route, run one timed simulation in the place that worries your team most. Measure the nurse-office distance, the cab-to-kit path, the phone-to-dispatch delay, and the interval between failed BLS and second-line deployment. Re-draw the deployment radius from those numbers, not from the building map.
Download the Remote & Mobile Readiness Toolkit
When help may be minutes away, readiness has to be planned before the emergency.
Download the Remote & Mobile Airway Safety Readiness Toolkit to map delays, assign roles, plan equipment access, and prepare your team for choking emergencies in rural, mobile, or field-based environments.
What did the ACS 2025 rural EMS analysis show?
The ACS analysis reported that rural total EMS call times averaged 92.8 minutes compared with 74.1 minutes nationally, with even longer times for high-acuity and specialty-center transports.
Why do rural EMS delays matter so much for airway emergencies?
Complete airway obstruction uses a much shorter clock than many other emergencies. Older national EMS research identified airway occlusion as one of the conditions where even modest delay can be life threatening.
What did DEN250012 change for second-line airway planning?
DEN250012 created 21 CFR 874.5400 for a suction anti-choking device as a second-line treatment after unsuccessful use of a basic life support choking protocol. It created a lawful federal category. It did not replace first-line BLS.
What does California AB 645 add to this discussion?
AB 645 requires California public safety agencies that process 911 medical calls to provide prearrival medical instructions by January 1, 2027, including airway and choking instructions. It shows how dispatcher-guided care can help bridge long arrival windows.
Why does the 20.5 kPa versus 8.2 kPa pressure comparison matter?
It shows that an authorized device and a counterfeit device do not operate inside the same physical performance range. The difference does not prove clinical success by itself, but it does matter when procurement teams evaluate backup devices for remote environments.
1) American College of Surgeons, 2025 Rural EMS Analysis
2) JAMA Surgery / NIH PMC EMS response-time analysis
3) FDA De Novo order DEN250012
4) Resuscitation Plus 2025 negative-pressure comparison
5) Trials 2023 simulated-use study
6) California AB 645 bill text
This article is for educational and operational planning purposes only. It does not provide medical or legal advice. Airway emergencies require immediate first-line response, activation of 911, and compliance with current American Heart Association or Red Cross guidance, local EMS protocols, and applicable federal and state requirements. Second-line devices should only be considered within their lawful intended use.




















