R&D Manager & Emergency Preparedness Specialist at Fitiger Life LLC
Medically Reviewed by Travis Brecka Captain & Critical Care Paramedic
|
• Bedside clinical swallowing assessment may miss up to 50% of silent aspiration cases in the literature. A resident can look calmer after rescue and still be entering a dangerous recovery path. |
|
• VFSS and FEES remain the widely used gold-standard tests for silent aspiration. Bedside screens and cough reflex testing can support triage, but they don't close the case when suspicion stays high. |
|
• VFSS-based studies cited in nursing-home dysphagia literature estimate aspiration prevalence at roughly 43% to 51% in people with dysphagia. Older adults with frailty, neurologic disease, or poor oral health face a tighter safety margin. |
|
• For facilities, the first 72 hours after rescue should be treated as a structured observation window. The airway may be open again while aspiration-related inflammation, cough change, oxygen drift, fever, or confusion are just beginning. |
A resident may look better and still be heading toward trouble. Aspiration means food, liquid, secretions, or gastric contents enter the airway below the vocal folds. Silent aspiration is harder operationally because it may leave no strong cough or dramatic bedside cue. Older adults with dysphagia, frailty, dementia, stroke, Parkinsonian changes, or poor dentition carry that risk into the hours after the event, not just the minute of obstruction.
In long-term care, the dangerous assumption is simple: the object came out, so the case is over. It often isn't. The event may already have shifted from airway obstruction to airway contamination, fatigue, residue, reduced intake, or early pulmonary inflammation.
It rarely announces itself cleanly. A resident may clear the throat over and over after the meal. Voice quality may sound wetter. Cough may become weaker instead of stronger. Appetite drops. Fatigue rises. The person who usually finishes the tray starts leaving food behind. A day later, oxygen saturation trends down, sputum changes, fever appears, or confusion shows up before anyone says the word 'aspiration.'
Older adults don't always present with loud respiratory distress. MedlinePlus notes that aspiration pneumonia can show up with cough, foul or discolored sputum, wheeze, shortness of breath, fatigue, fever, and confusion. That symptom pattern is exactly why facilities need a post-rescue script instead of treating the event as finished once breathing improves.
I wouldn't describe 72 hours as a universal law written the same way in every guideline. I would describe it as the right operational watch window for facilities that don't want the post-rescue story to disappear.
The first few hours matter because the resident may still have residue, altered voice, fatigue, or immediate respiratory irritation. The next day matters because deterioration is often picked up through trend instead of one dramatic finding. By 48 to 72 hours, the team should know whether symptoms are resolving, whether reassessment is needed, and whether the event belongs in the facility's quality-improvement workflow.
The common error is ending the workflow too early. Three things usually follow. Oral intake resumes without enough thought. The next shift doesn't know exactly what to watch. Documentation captures the rescue but not the recovery path. A post-event script prevents clinical oversight during shift changes.
Nursing-home dysphagia literature keeps pointing to the same protective measures: reassessment, upright positioning, texture modification when appropriate, feeding assistance, slower meal pace, environmental control, and oral-care routines. Facilities that rescue well but monitor poorly are still leaving risk on the table.
This framework doesn't replace physician orders, nursing judgment, speech-language pathology evaluation, or local escalation rules. It gives the team one disciplined way to keep the resident visible after the obstruction clears.
|
Time window |
What the team should watch |
Why it matters |
|
0 - 4 hours |
Baseline oxygen saturation, work of breathing, voice quality, cough quality, visible fatigue, oral-intake hold or review per facility protocol. |
Catches immediate irritation, residue concern, fatigue, or an unsafe return to PO. |
|
4 - 24 hours |
New cough, wet voice, throat clearing, wheeze, respiratory-rate trend, appetite drop, rising suction needs, mental-status change. |
This is where 'seems fine now' can turn into the start of aspiration-related decline. |
|
24 - 48 hours |
Temperature trend, sputum change, oxygen need, confusion, weakness, clinician reassessment, swallow-risk review. |
Helps separate transient irritation from a worsening pulmonary or swallowing picture. |
|
48 - 72 hours |
Symptom resolution or persistence, need for imaging or referral, care-plan change, incident review trigger, QAPI follow-up. |
Closes the loop between bedside event and facility-level learning. |
The rescue itself needs role clarity. The recovery period does too. Too many teams chart the obstruction and nobody owns the next 24 hours.
|
Role |
Primary job |
Operational value |
|
Lead clinical watch |
Owns respiratory and swallowing observation after the event and decides what needs escalation under facility protocol. |
Keeps the resident clinically visible instead of assuming the obstruction phase was the whole event. |
|
Meal and swallow protection |
Prevents a casual return to routine intake, briefs aides and family, and aligns meal handling with orders or protocol. |
Stops the resident from sliding back into the same conditions that made the event unsafe. |
|
Documentation and escalation |
Captures the timeline, rescue method, post-event symptoms, reassessment plan, and who owns the next check. |
Prevents handoff loss and gives the case a clean path into incident review or QAPI. |

A resident who keeps coughing, sounds wet, struggles with swallowing, shows respiratory symptoms, or repeatedly triggers concern after the event should not be treated as 'resolved just because the object came out.' Bedside observation and cough-based screening can help triage. They don't rule silent aspiration out when suspicion stays high. VFSS and FEES remain the widely used gold-standard assessments.
Fitiger belongs in the rescue layer as an adult anti-choking device option, but the authority move is not to stop there. FDA's March 4, 2026 safety communication says established choking-rescue protocols come first and an authorized anti-choking device may be used as a second option only after standard protocols are unsuccessful. That matters during the obstruction phase. The recovery phase still needs monitoring, documentation, and escalation discipline.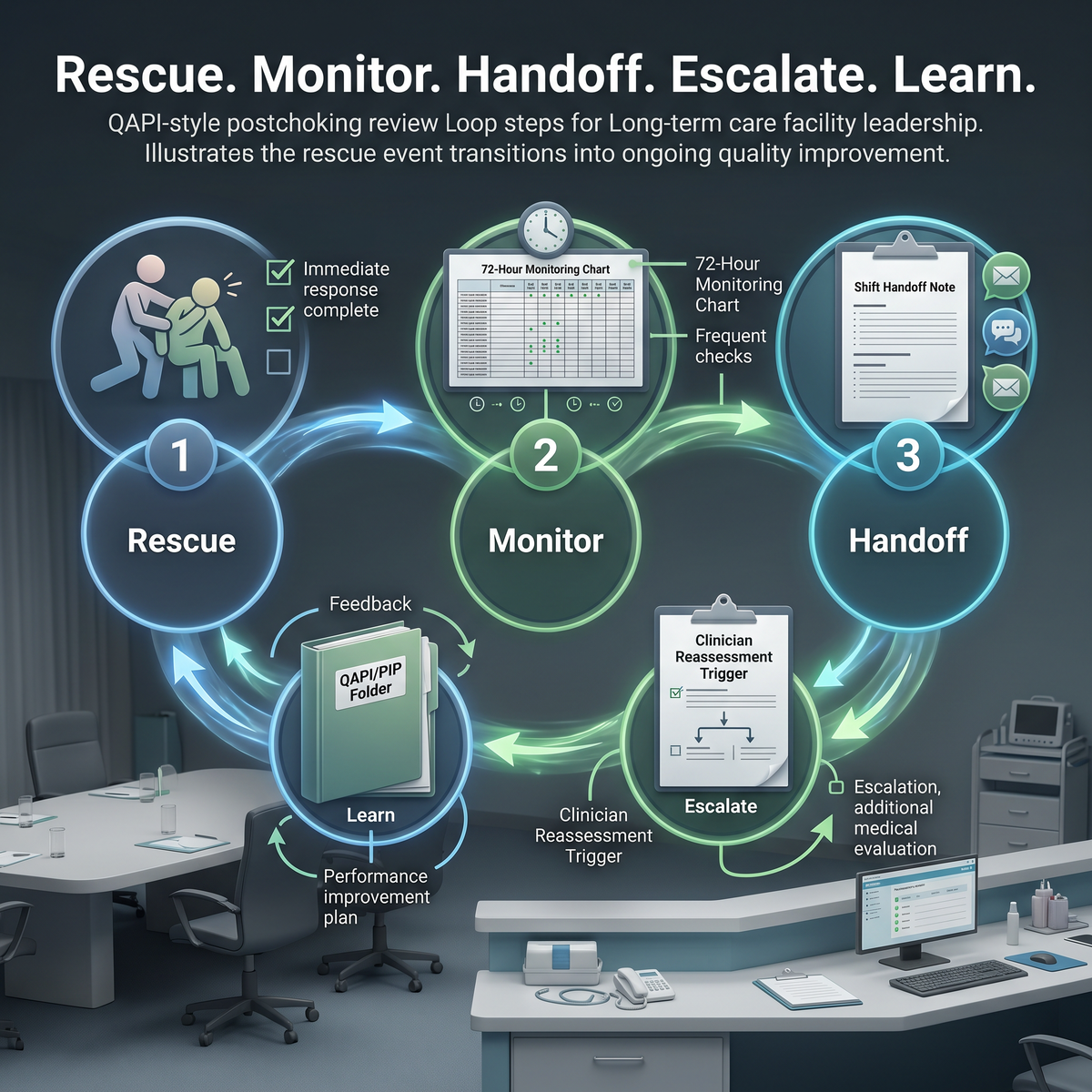
A facility that uses a second-line rescue device and then has no post-event pathway is only solving half the problem. A better system gets through the obstruction, then keeps the resident visible long enough to catch what the obstruction may already have set in motion.
Add post-choking monitoring to the facility's next PIP review instead of treating it as a bedside-only event. A simple self-audit after each rescue can expose the real weak points.
☐ Did the team document who owned the next 24 hours of respiratory and swallowing observation?
☐ Did oral intake resume under a clear review process instead of routine habit?
☐ Was there a defined trigger for clinician reassessment, imaging, or SLP referral if symptoms persisted?
☐ Did the next shift receive a clean handoff with specific watch items instead of a vague note that the resident was 'better'?
☐ Was the event logged in a way that can feed QAPI trend review, not just incident storage?
The dangerous version of this event isn't always the one where the rescue fails. Sometimes it's the one where the rescue works, everyone exhales, and the team stops watching too soon. Long-term care teams don't need a bigger slogan here. They need a sharper workflow: rescue, monitor, hand off, escalate, and learn from the event.
No. The airway may be open again while aspiration-related risk remains. Silent aspiration and aspiration pneumonia can still develop after the object is removed, especially in older adults with dysphagia, frailty, or neurologic disease.
Not reliably. Bedside screening can support triage, but VFSS and FEES remain the widely used gold-standard assessments when suspicion stays high.
Watch respiratory effort, cough quality, voice quality, oxygen trend, fever, sputum change, appetite, fatigue, and new confusion. In older adults, pneumonia may present less dramatically than expected.
Reassessment, texture modification when appropriate, feeding assistance, upright positioning, environmental control during meals, and oral-care routines show up again and again in the nursing-home literature.
Yes. A choking rescue followed by aspiration concern should become part of incident review and performance improvement, not just a one-time note in the chart.
FDA Safety Communication
MedlinePlus: Aspiration Pneumonia
MedlinePlus: Dysphagia Tests
NIA: Care in the Last Stages of Alzheimer's Disease
Sun et al. 2025 systematic review and meta-analysis
Chen et al. 2021 scoping reviewThis article is for educational and preparedness purposes only. It's not medical advice and doesn't replace physician judgment, nursing assessment, speech-language pathology evaluation, emergency care, or local facility protocol.




















