In a real airway emergency, knowing something is wrong is only the beginning. Knowing exactly where it is happening is what determines how fast help arrives.
A student chokes in a hallway between classes. Someone triggers an alert. The office gets the message, then security, then a radio call goes out: 'near the science wing.' One staff member takes the wrong staircase. Another stops to ask which room. The adult at the scene keeps working, but the next layer of help is still trying to find the door.
Training stops at the door. If the backup team cannot find that door, the first minute is already gone.
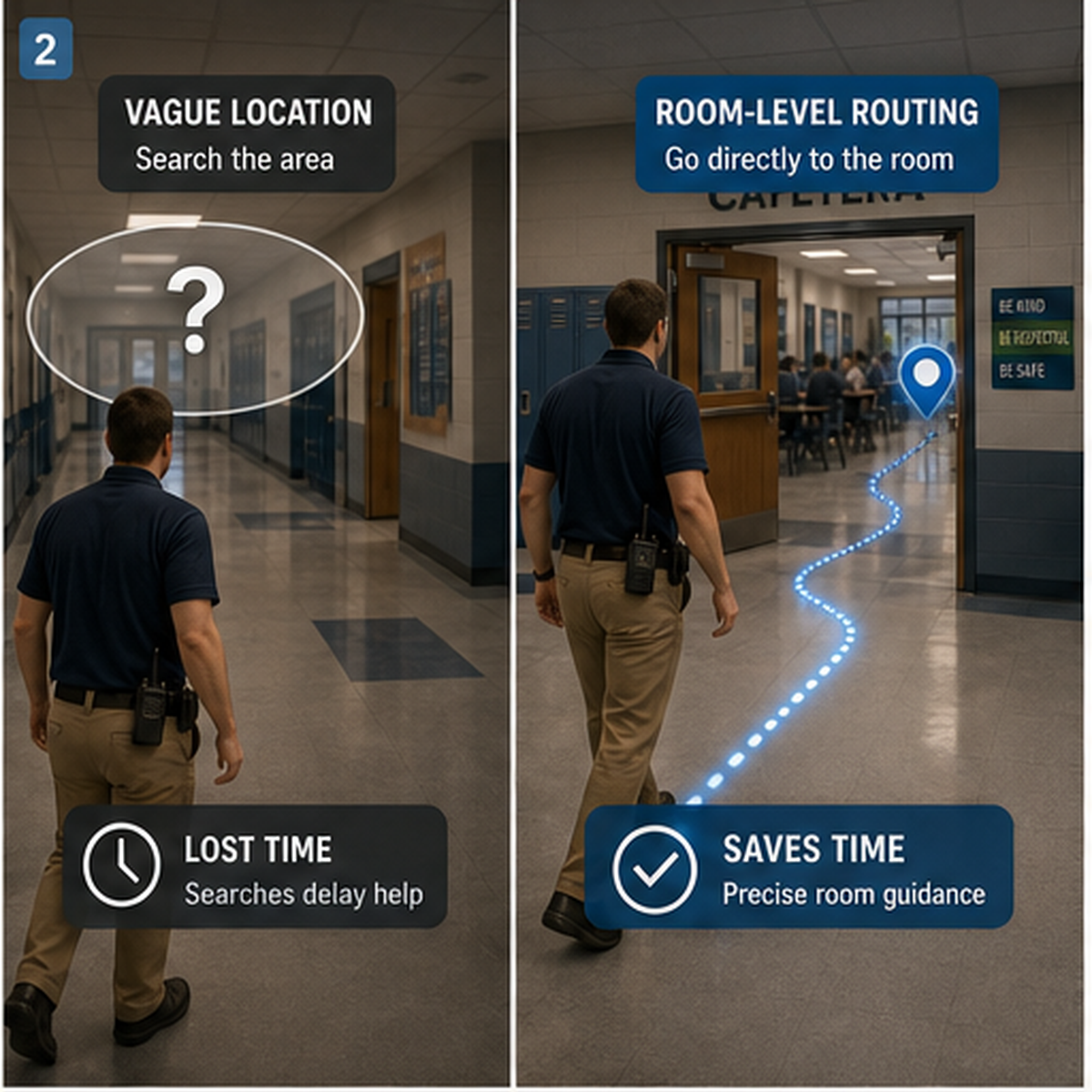
BLE indoor location reduces emergency delay by removing search time. Instead of relying on shouted directions, hallway guesses, or repeated radio clarification, the system identifies the room and routes support toward it. In a choking emergency, that allows the lead responder to stay with the victim and begin manual rescue while the rest of the response chain starts moving in the right direction.
'Near the cafeteria' is not a usable instruction when a child cannot speak and the nearest adult has already started the rescue sequence. Indoor emergencies break down on location more often than schools admit.
In a quiet office, a loose description may be enough. In a crowded school, clinic, or eldercare building, every extra question adds delay. Which hallway? Which door? Which floor? The responder on scene should not have to answer those questions while keeping both hands in the event.
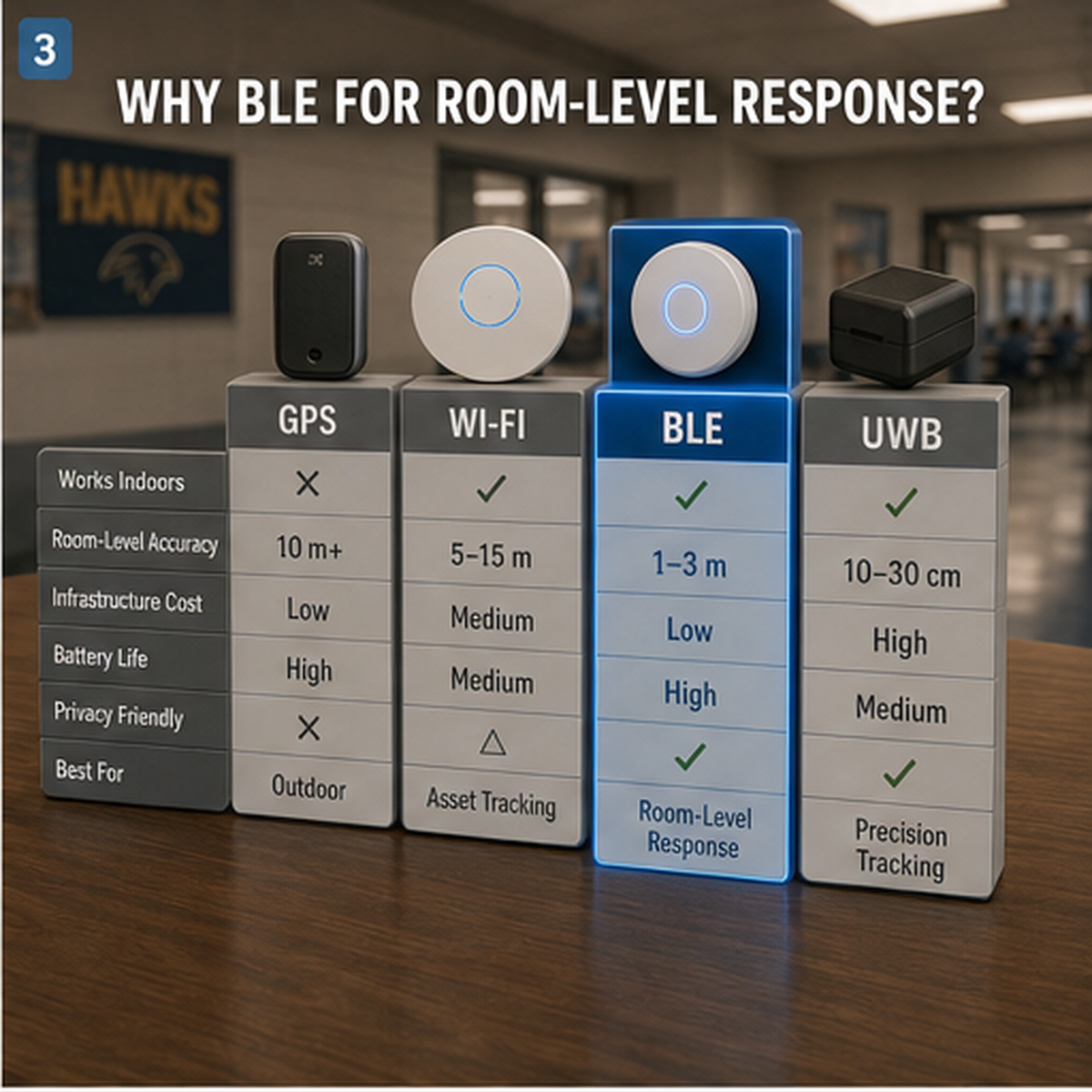
Several indoor positioning technologies can locate people inside buildings, but most institutions do not need lab-grade precision. They need room-level awareness that works at scale.
BLE fits that need well. Small, low-cost beacons can be distributed across rooms and hallways. A wearable badge or alert device detects nearby beacons and passes that information to the response system. In a crisis, room-level awareness is the only metric that matters. Centimeter precision is a luxury schools do not need if the system can get the next responder to the right door fast enough.
A severe choking event always runs on two tracks at once. One track is physical rescue at arm's reach. The other is the system moving support toward that rescue.
For a conscious child with severe foreign-body airway obstruction, the current first-line sequence is repeated cycles of 5 back blows followed by 5 abdominal thrusts until the object is expelled or the child becomes unresponsive. The American Red Cross teaches the same 5-and-5 structure for children. That consistency matters under stress.
BLE location does not replace first aid. It removes the search phase around first aid.
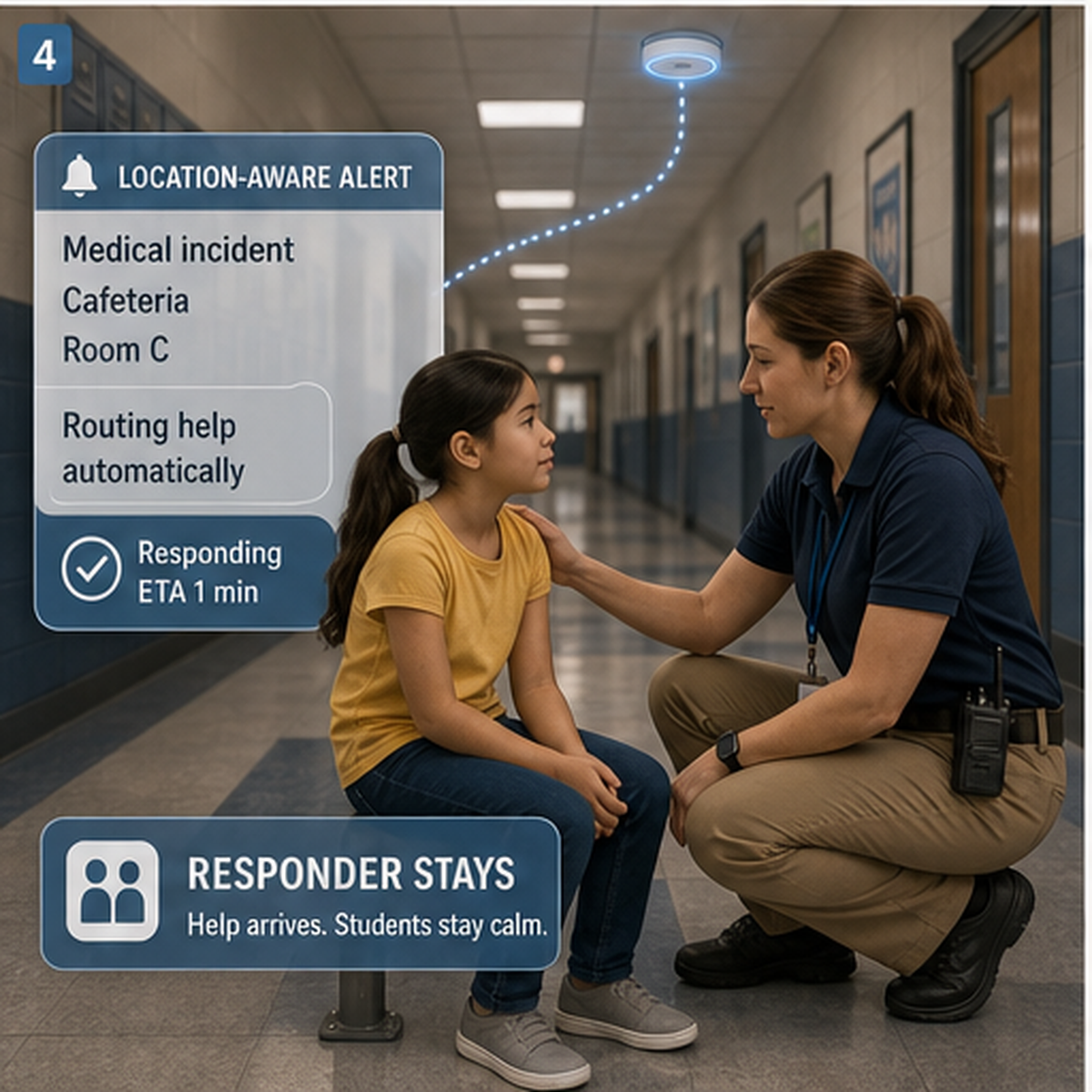
Without location-aware alerting, the adult closest to the victim faces a bad tradeoff almost immediately: keep performing the rescue sequence or leave the scene to get help. That rescuer's dilemma is where response systems quietly fail.
Indoor location changes that pressure. The responder stays in place. The system carries the location outward. Nearby trained staff, nurses, security, or administrators start moving toward a known room instead of a guessed area.
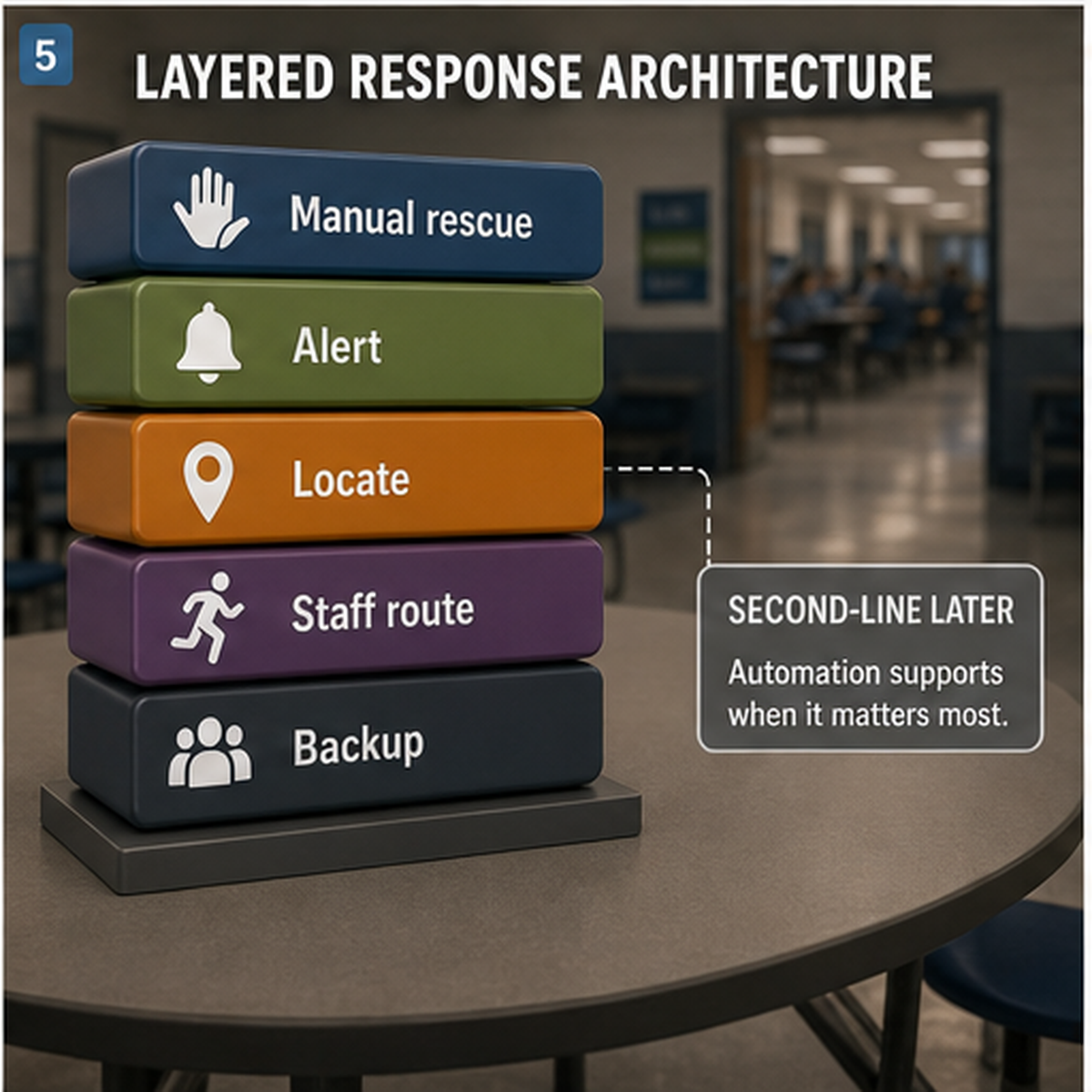
Indoor location works best when it is part of a larger response design. Manual rescue remains first-line. Alerting removes communication lag. Location removes search time. Staffing workflows determine who arrives next. Equipment staging determines what arrives with them.
Second-line suction devices sit later in that chain. FDA's March 4, 2026 De Novo decision created the Class II category 'suction anti-choking device as a second-line treatment' under 21 CFR 874.5400, product code QXN. In practical terms, these negative-pressure devices belong after unsuccessful use of a basic life support choking protocol, not before it.
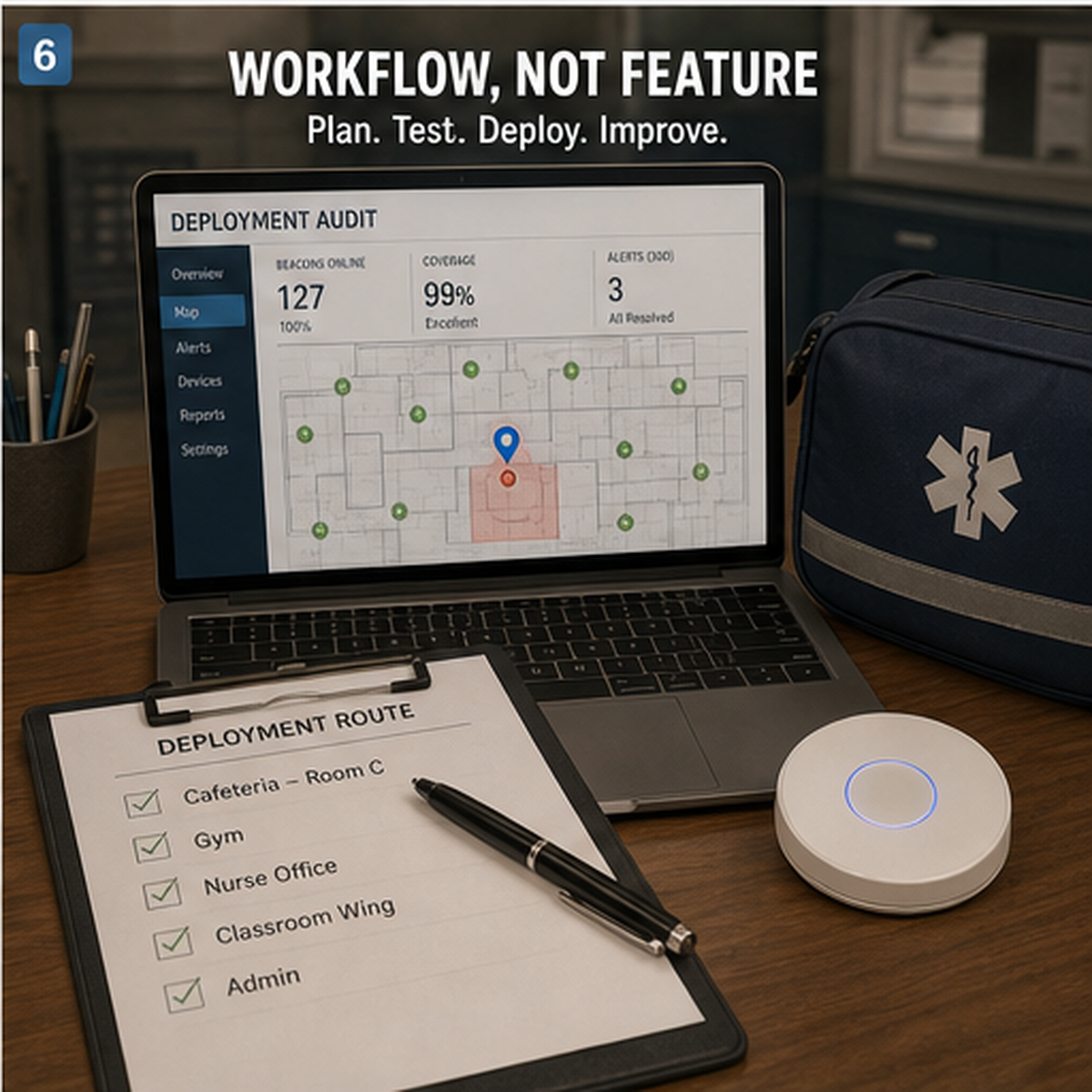
Indoor location does not automatically make response faster. It fails when schools treat it like a feature instead of a workflow. If the alert is not tied to the right response group, location data creates noise instead of speed. If staff are not trained to move on location-based alerts, the system only adds another dashboard. If emergency equipment is staged far from real activity zones, responders still arrive empty-handed.
Technology helps only when it shortens a real path inside the building.
Room-level indoor location is changing medical response in a quiet but important way. It does not replace judgment, first aid, or training. It removes wasted movement.
For schools and care environments, the practical question is simple: if a choking emergency starts in the loudest, busiest part of the building, can the next layer of help find the room without asking anyone to leave the scene? If the answer is no, the response system is still slower than the emergency.
GPS performs poorly indoors because walls, metal structures, and building geometry degrade the signal. BLE is easier to deploy room by room and can provide the kind of room-level location awareness that matters in first-minute medical response.
No. BLE location removes search time. It does not replace the physical response. For severe choking in a conscious child, the first-line sequence remains 5 back blows followed by 5 abdominal thrusts until the object is expelled or the child becomes unresponsive.
They are second-line backup devices, not first-line rescue tools. FDA's Class II QXN category defines them for use after unsuccessful use of a basic life support choking protocol.
Treating location as a feature instead of a workflow. If the alert does not reach the right people, if staff do not move on it, or if the equipment is still staged far away, the system will not shorten the first minute in a meaningful way.
American Heart Association - Supports the current child severe foreign-body airway obstruction sequence of 5 back blows followed by 5 abdominal thrusts
American Red Cross - Supports the same 5-back-blows and 5-abdominal-thrusts first-aid sequence for children
FDA De Novo decision DEN250012 - Supports the Class II QXN category and second-line role of suction anti-choking devices after unsuccessful basic life support choking protocol
FDA safety communication - Supports current public guidance that established choking rescue protocols should come first
BLE indoor positioning study - Supports BLE as a practical low-cost indoor positioning approach for room-level awareness in real deployments
Indoor localization review - Supports practical tradeoffs between BLE, Wi-Fi, GPS, and UWB for indoor positioning systems
This article is for educational and emergency preparedness purposes only. It is not medical advice, diagnosis, or treatment. In a choking emergency, begin established first-aid measures immediately, call 911 or your local emergency number, and follow current accredited guidance. Any suction anti-choking device should only be considered as a second-line measure after unsuccessful standard choking rescue protocols, consistent with current FDA public guidance.




















