
Older adults with dysphagia face choking risk when food texture no longer matches their swallowing ability. Tough meat, dry bread, mixed-texture soup, raw vegetables, nuts, and sticky foods can become unsafe. Safer meals start with texture modification, slower pacing, upright seating, caregiver awareness, 911 readiness, and second-line backup only after first-line rescue fails.
For a household checklist, see Fitiger's child and home choking safety readiness plan.
The first warning sign is not always a dramatic choking event.
Sometimes an older adult quietly stops eating steak. Bread comes back untouched. Pills take longer. Salad is pushed around the plate. A caregiver hears a wet cough after dinner and assumes it is just age. A daughter notices her father drinking water after every bite but does not know whether to worry. In a nursing home dining room, one resident keeps pocketing food in the cheek while everyone else is focused on the next tray.
That is how dysphagia often enters the room: quietly, meal by meal.
Dysphagia means difficulty swallowing. It can happen after stroke, Parkinson's disease, dementia, frailty, head and neck conditions, medication effects, dental problems, or general muscle weakness. For families searching "foods to avoid with dysphagia" or "older adults choking risk foods," the real question is usually not just which foods are dangerous. It is how to tell when the person's eating ability has changed.
Older adults do not all need the same diet. A food that is easy for one person may be unsafe for another. The most useful approach is not fear. It is matching food texture to the person in front of you.
A dysphagia safe eating guide should begin with four practical questions:
Can the person chew this food fully?
Does the food stay moist enough to swallow?
Does the texture stay consistent from bite to bite?
Can the person eat it without coughing, fatigue, pocketing, or needing repeated sips to force it down?
If the answer is no, the food needs to change before the emergency happens.
Choking prevention for toddlers is often about food size and shape. Choking prevention for older adults is usually more complex.
The airway is the same critical passage, but the risk factors are different. Older adults may have weaker cough, slower reflexes, reduced saliva, loose dentures, missing teeth, neurological disease, or reduced coordination between chewing, breathing, and swallowing. A person may also be taking medication that dries the mouth or causes drowsiness. If they live alone or eat with limited supervision, recognition delay becomes part of the risk.
This is why "senior choking prevention" cannot be reduced to "cut food smaller."
Cutting helps, but texture matters more. A small dry piece of bread can still become a sticky mass. Finely chopped salad can still scatter in the mouth. Rice can separate into grains. Mixed-texture soup can ask the mouth to manage liquid and solid at the same time. Tough meat can require more chewing strength than the person has.
In senior care, the most dangerous food is often the one that looks normal to the person serving it.
A dysphagia-informed mealtime plan should consider:
| Moisture. | Softness. | Particle size. |
| Chewing demand. | Mixed textures. | Pacing. |
| Posture. | Fatigue. | Supervision level. |
| Clinician guidance. |
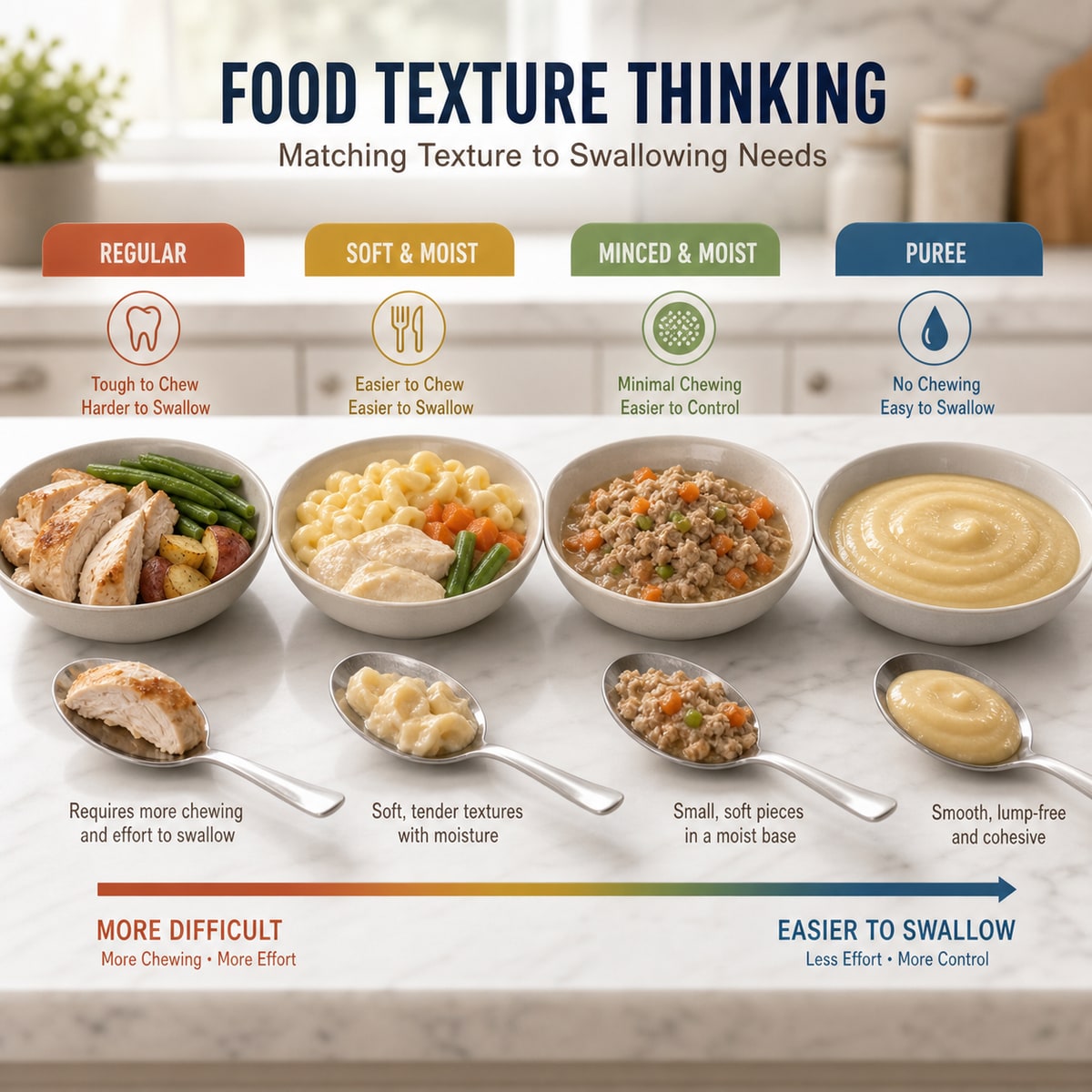
That is also why IDDSI-style texture thinking matters. IDDSI, the International Dysphagia Diet Standardisation Initiative, gives clinicians and care teams a shared language for food and drink texture levels. Families do not need to become texture experts overnight, but they should understand the principle: safer meals are not just about what food is served. They are about how that food behaves in the mouth.
For care teams, food texture and handoff planning helps turn repeated mealtime observations into safer kitchen decisions.

Instead of treating this as a generic "do not eat" list, use it as a conversation starter with clinicians, caregivers, and family members. If an older adult coughs, tires, avoids, pockets, or struggles with one of these foods, the answer is not embarrassment. The answer is adjustment.
Tough meat is one of the most common high-risk foods for older adults because it demands strong chewing and saliva. Steak, pork chops, dry chicken breast, sausage skin, and jerky can form large, poorly chewed pieces.
Someone with dentures may chew less effectively. Someone with dry mouth may not form a smooth bolus. Someone with Parkinson's disease or post-stroke swallowing changes may fatigue before the meal is over.
Safer approach: cook meat until tender, add gravy or sauce, shred or mince, remove tough edges, serve smaller portions, and avoid dry reheated cuts. If chewing remains difficult, ask a clinician or speech-language pathologist whether a texture-modified diet is needed.
The goal is not to remove protein. The goal is to make the protein manageable.
Bread can be deceptive. It looks soft, but dry bread can clump, stick, and become hard to move through the mouth. Rolls, thick sandwiches, toast, biscuits, and bagels may become especially difficult when saliva is low.
Many older adults compensate by drinking water after every bite. That may help occasionally, but repeated "washing down" can be a warning sign. Food that needs to be forced down may not be the right texture.
Safer approach: choose softer breads, remove tough crusts if needed, add moisture, cut smaller pieces, avoid oversized sandwiches, and watch for coughing or wet voice after swallowing.
Rice creates a different problem. It does not behave like one soft piece. It separates into small grains that can scatter through the mouth and throat. Dry rice, fried rice, quinoa, couscous, and similar grains may become difficult for people with poor bolus control.
Safer approach: serve rice moist with sauce, choose softer preparations, slow the pace, and avoid dry mixed grain bowls if the person struggles.
Caregivers should watch for throat clearing after rice dishes. It may look minor, but repeated coughing tells you the texture is not working well.
Soup seems safe because it is soft. Mixed-texture soup can be harder than it looks because the person must manage thin liquid and solid chunks at the same time.
Chicken noodle soup, vegetable soup, minestrone, cereal with milk, and broth with meat pieces can create timing problems for people with dysphagia. The liquid moves quickly, while the solid pieces need chewing.
Safer approach: use a consistent texture when needed. That may mean blending, thickening under clinician guidance, or choosing soft solids without thin liquid mixed in. Do not thicken liquids casually without medical guidance; thickened liquids are clinical tools, not kitchen guesses.
Raw produce is healthy, but chewing demand matters. Carrots, celery, apple chunks, firm pears, raw broccoli stems, and similar foods can break into hard pieces.
For older adults with dentures, poor chewing strength, or delayed swallowing, firm produce may be too much work.
Safer approach: steam vegetables, grate carrots, stew apples, slice very thinly, peel when helpful, and serve with moisture.
Nutrition still matters. The safer version of a food often keeps the nutritional value while reducing the mechanical burden.
Salad can be one of the most frustrating foods for older adults with swallowing difficulty. Lettuce, spinach, kale, and leafy greens can spread across the mouth, stick to the palate, or require repeated chewing. Stringy greens can be hard to form into a safe swallow.
Safer approach: chop finely only if that truly helps the person; otherwise cook greens until soft. Add moisture. Avoid large leaves. Watch for pocketing or leftover pieces in the mouth.
A salad may look light, but it can be a complex swallowing task.
Nuts and seeds are hard, small, and easy to lose control of in the mouth. Trail mix adds multiple textures: hard nuts, chewy dried fruit, chocolate pieces, seeds, and sometimes sharp fragments.
This kind of mixed handful eating is especially risky when someone eats while watching TV, talking, or walking around the kitchen.
Safer approach: avoid whole nuts if chewing or swallowing is impaired. Ask a clinician about safer forms if nuts are important to the person's diet.
Thick peanut butter can coat the mouth, stick to the palate, and form a dense mass. The same concern applies to thick nut butters, sticky protein spreads, caramel-like foods, and some dense snack pastes.
Safer approach: spread very thinly, mix into softer foods, or use alternatives recommended by a clinician. Avoid spoonfuls.
Sticky foods are often underestimated because they are soft. Soft does not always mean safe.
Dry snacks break apart and absorb moisture. Crackers, chips, rice cakes, cookies, and crisp breads may create crumbs that are hard to control, especially for someone with dry mouth.
Safer approach: soften when appropriate, serve with moisture, use small portions, and avoid fast snacking while distracted.
For older adults living alone, dry snack foods can be risky because they are often eaten casually and without preparation.
Pineapple, citrus membranes, celery strings, tough mango, and fibrous vegetable pieces can be hard to break down. The person may chew and chew without forming a smooth swallow.
Safer approach: choose softer fruit, cut across fibers, remove stringy parts, stew or blend when needed.
Families often worry that a dysphagia-friendly meal will feel like a loss. That fear is real. Food is identity, memory, control, pleasure, and dignity. Nobody wants to be told that the foods they love are now unsafe.
A better approach is to improve the meal rather than simply restrict it.
Tough steak can become slow-cooked shredded beef with sauce.
Dry chicken can become moist chicken salad with finely chopped pieces if the person can manage that texture.
Raw apples can become warm cinnamon apples.
Dry toast can become soft bread with moisture.
Large salad can become cooked greens.
Rice can become a moist risotto-style dish if appropriate.
The phrase "texture modified diet" sounds clinical. In a home kitchen, it can mean cooking food in a way that respects the person's current body.
For care facilities, the same idea matters. A dysphagia safe eating guide should not only say "avoid." It should offer alternatives that preserve dignity.

Do not wait for a full choking emergency to adjust food.
If any of these signs repeat, the meal routine deserves review:
| Coughing during meals. | Throat clearing after swallowing. | A wet or gurgly voice. |
| Food left in the cheeks. | Food falling from the mouth. | Needing many sips to swallow. |
| Avoiding certain foods. | Taking much longer to eat. | Fatigue before finishing. |
| Unexplained weight loss. | Recurring chest infections. | Fever or confusion after suspected aspiration. |
| Shortness of breath after meals. |
Some symptoms may point to aspiration risk, not just choking risk. Aspiration means food, liquid, saliva, or stomach contents may enter the airway. Aspiration pneumonia can show up with respiratory and systemic symptoms, and older adults may not always present in obvious ways. Repeated coughing or wet voice after meals should not be brushed off as "just getting older."
A clinician should guide any major diet change. A speech-language pathologist can evaluate swallowing and recommend safer texture levels when needed.
This food-focused guide should sit beside the broader kitchen safety for seniors living alone plan, because texture choices and emergency access work together.
A home plan for older adults with dysphagia should be built around the dining spot.
Start with posture. The person should sit upright, not reclined. Feet should be stable. The plate should be close. Lighting should be good enough to see food clearly. Distraction should be reduced.
Then adjust the meal:
Small bites.
Slow pace.
One texture at a time when needed.
Moist foods.
Avoid rushed talking while chewing.
Rest breaks if fatigue appears.
Dentures checked.
Water available, but not used to force unsafe food down.
If the person lives alone, add response planning:
| Phone within reach. | Emergency contacts set. |
| Door access plan. | Address visible. |
Neighbor or family check-in if risk is high.
A second-line anti choking device only if appropriate, familiar, and stored near meals.
For families searching "choking rescue device for elderly" or "anti choking device for home," this is the part that matters most. A device should not become a substitute for safer meals or first-line rescue. It should be a backup layer after prevention, recognition, and standard response.

In assisted living, nursing homes, memory care, adult day programs, and home health settings, choking prevention becomes operational.
The person eating may have a care plan. The kitchen may have texture orders. Staff may rotate. Family members may bring outside food. Dining rooms may be noisy. A resident may trade food or pocket food. Someone may eat too quickly because the table is being cleared.
Senior care teams need a shared system:
| Document diet texture needs. | Communicate swallowing warnings during shift changes. |
| Monitor dentures and oral discomfort. | Watch high-risk foods. |
| Control outside snacks. | Train staff in choking recognition. |
Call 911 early when severe choking occurs.
Use first-line rescue according to training.
Stage any second-line backup device where policy allows.
Document incidents and near misses.
The phrase "choking safety in senior care" should mean more than buying equipment. It should mean building a meal environment where staff can see risk before the airway is blocked.
A resident who coughs every time they eat bread is giving the system a warning.

This article is about food, but emergency sequence still belongs here.
If severe choking occurs, call 911 immediately or send someone to call. Begin trained first-line choking rescue. If the person becomes unresponsive, begin CPR according to training and dispatcher guidance.
A suction anti choking device may be considered only as second-line backup if standard rescue steps are unsuccessful and the person fits the current product instructions. It should not delay 911, back blows, abdominal thrusts or chest thrusts when indicated, CPR, or EMS.
For Fitiger, the responsible role is clear: preparedness support inside a larger choking response system.
EasyPumpVac may be better suited for home, car, bedside, and senior living standby because its easier-pull mechanical design may reduce handling burden for older adults, caregivers, and users with limited hand strength.
FoldPumpVac may be better suited for portable readiness, travel, caregiver bags, vehicle kits, and movement between homes or care settings.
Neither product replaces food texture planning, dysphagia evaluation, first-line choking rescue, or emergency medical care.
A second-line device stored well can reduce retrieval delay. A device used first can create delay. That difference has to stay visible.
Families and facilities comparing devices should review Fitiger scientific evidence before deciding how second-line backup fits into a written response system.
Use this checklist when preparing meals for an older adult with suspected or confirmed swallowing difficulty.
|
Mealtime question |
Safer direction |
|---|---|
|
Is the food tough or chewy? |
Tenderize, shred, mince, moisten, or replace |
|
Is the food dry? |
Add sauce, broth, moisture, or choose softer food |
|
Does it scatter into small pieces? |
Avoid or use a more cohesive texture |
|
Is it sticky? |
Thin it, mix it, or avoid spoonfuls |
|
Does it mix liquid and chunks? |
Use a consistent texture if needed |
|
Is the person coughing during meals? |
Pause and seek clinical guidance if repeated |
|
Are dentures loose or painful? |
Address dental fit before blaming the food |
|
Is the person eating alone? |
Add phone access and emergency plan |
|
Is food being pocketed? |
Reduce bite size and seek swallowing evaluation |
|
Is there a backup device? |
Keep it visible, complete, and second-line only |
This table is not a medical prescription. It is a way to notice mismatch.
Older adults with dysphagia do not need panic at the table. They need food that matches their swallowing ability, people who notice small changes, and a response plan that does not wait for collapse.
The safest meals are often quiet improvements: meat cooked softer, bread served with moisture, raw vegetables softened, rice made less dry, a phone moved closer, dentures checked, coughing taken seriously.
If a Fitiger device is present, it belongs near the meal area as a second-line backup, not as a replacement for safer food, first-line rescue, 911, CPR readiness, EMS, or clinical care.
Choking prevention for older adults is not one decision. It is a habit repeated at every meal.
For related planning context, review the child and home choking safety readiness plan.
Foods that often raise risk include tough meats, dry bread, rice, raw carrots, apple chunks, nuts, seeds, thick peanut butter, leafy salads, mixed-texture soups, dry crackers, chips, and stringy fruit. Risk depends on the person's chewing, saliva, dentures, fatigue, and swallowing ability.
Dysphagia means difficulty swallowing. It can happen after stroke, Parkinson's disease, dementia, frailty, head and neck conditions, medication effects, or other medical issues. Dysphagia can increase choking and aspiration risk, so repeated symptoms should be evaluated by a clinician.
Warning signs include coughing during meals, wet or gurgly voice, food pocketing, needing extra water to swallow, avoiding certain foods, long mealtimes, fatigue, weight loss, repeated chest infections, or breathing symptoms after meals.
Yes, dry foods can be risky for people with dysphagia or dry mouth. Bread, crackers, rice cakes, chips, dry rice, and cookies may crumble, clump, or become hard to swallow. Moisture and softer textures can reduce risk.
Only under clinician guidance. Thickened liquids are sometimes recommended after swallowing evaluation, but they should not be guessed at home. The wrong thickness can create other problems.
Rice may be difficult for some people because grains separate in the mouth and throat. Moist rice preparations may be easier than dry rice, but the safest choice depends on the person's swallowing evaluation and tolerance.
A suction anti choking device may be considered as a second-line backup only after standard choking rescue steps are unsuccessful and only if the device fits the current instructions for use. It should not replace safer food textures, supervision, 911, first-line rescue, CPR, EMS, or clinical care.
EasyPumpVac may be better for home, bedside, car, and senior living standby because its easier-pull design may reduce handling burden. FoldPumpVac may be better for portable placement, travel, caregiver bags, and vehicle kits. Both remain second-line backup devices.
Senior care facilities can reduce choking risk by documenting diet texture needs, monitoring swallowing warning signs, training staff, controlling outside food, keeping residents upright, slowing meals, assigning response roles, calling 911 early, and documenting choking or near-miss events.
Call 911 immediately if the person cannot speak, cough effectively, breathe, or is losing consciousness. Begin trained first-line choking rescue while help is on the way. If the person becomes unresponsive, begin CPR according to training and dispatcher instructions.
IDDSI - International Dysphagia Diet Standardisation Initiative - Supports standardized thinking around food texture and liquid thickness for dysphagia care.
MedlinePlus Swallowing Difficulty - Supports general medical education around dysphagia symptoms and swallowing problems.
MedlinePlus Aspiration Pneumonia - Supports awareness of symptoms that may follow aspiration, including cough, breathing changes, fever, fatigue, and confusion.
American Red Cross Adult and Child Choking First Aid - Supports first-line choking response education for adults and children.
FDA Choking Rescue Protocols Safety Communication - Supports the first-line rescue first, second-line anti-choking device backup only after standard protocols are unsuccessful.
This article is for general education and emergency preparedness only. It is not medical advice, diagnosis, or treatment. Older adults with repeated coughing, swallowing difficulty, suspected dysphagia, aspiration symptoms, weight loss, recurring chest infections, or sudden eating changes should be evaluated by a qualified clinician. In a choking emergency, call 911 or your local emergency number immediately and follow dispatcher instructions. Any anti choking device should be treated as a second-line backup, not a replacement for safer food preparation, clinical care, first-line rescue, CPR, EMS, or professional medical treatment.




















