|
The comparison is not brand familiarity. It is whether a second-line device can reduce retrieval delay inside the first 4 minutes while preserving AHA first-line action. FoldPumpVac should be evaluated for compact staging, seal integrity, material evidence, and second-line placement, not as a replacement for manual rescue. Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions. |
LifeVac is the better-known name in the suction anti-choking device category. Fitiger FoldPumpVac enters the same buyer conversation from a different direction: response geometry. A device stored too far from the meal, care room, bus kit, or school cafeteria is not absent from inventory. It is absent from the first minutes of response.
For Fitiger, the disciplined comparison is not LifeVac versus FoldPumpVac as two product photos. It is central storage versus point-of-need staging, brand awareness versus retrieval latency, and generic suction language versus a defined second-line response boundary.
A second-line suction device should never be the first move. Current choking response guidance places first-line action before device use. For responsive adults and children with severe foreign-body airway obstruction, the 2025 AHA algorithm uses repeated cycles of 5 back blows followed by 5 abdominal thrusts until the object is expelled or the person becomes unresponsive. When the rescuer cannot encircle the abdomen, chest thrusts become the practical first-line alternative. Infants use 5 back blows and 5 chest thrusts, not abdominal thrusts.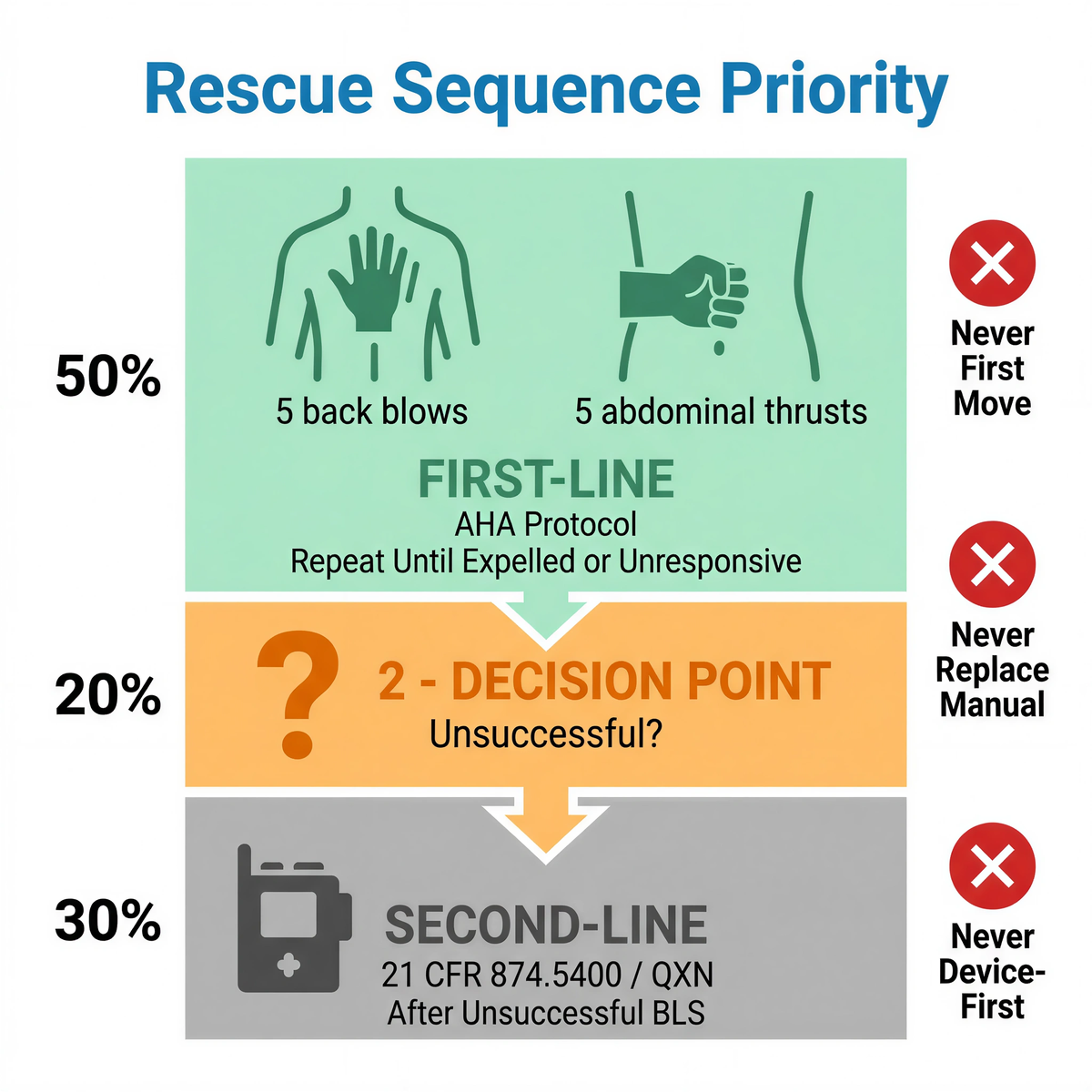
The FDA 2026 framework reinforces that order. The De Novo order for DEN250012 created 21 CFR 874.5400 for a suction anti-choking device as a second-line treatment, with product code QXN, after unsuccessful use of a basic life support choking protocol. That boundary is the comparison floor for every product in the category.
Survival redefines the comparison: brand familiarity is an administrative metric, while retrieval latency is a biological one. The device that looks best online may still be poorly placed, poorly understood, or too slow to reach.
|
Comparison point |
LifeVac buyer question |
FoldPumpVac buyer question |
Why it matters |
|
Second-line boundary |
Does the exact product documentation preserve use only after unsuccessful first-line rescue? |
Does Fitiger present FoldPumpVac as backup inside the same sequence, not as device-first care? |
Prevents delay of established choking protocols. |
|
Staging geometry |
Where does the device live before the emergency? |
Can folding design support point-of-need staging near meals, travel kits, school zones, or care rooms? |
Distance from the device becomes time lost. |
|
How does the mask seal across real faces and positions? |
Are mask material, seal surface, and replacement path clearly described? |
Suction output depends on seal integrity. |
|
|
Handling path |
How many actions happen under stress? |
Can a non-medical user understand retrieval, mask placement, and pull sequence within training? |
Stress reduces recall and fine motor control. |
|
Evidence boundary |
What evidence supports performance and what does it not prove? |
Can Fitiger separate material, bench, storage, and post-use signals without overstating outcome? |
Credibility depends on not turning tests into clinical promises. |
LifeVac has a public FDA De Novo reference point. That does not make every similar-looking suction product equivalent, and it does not automatically answer the status of a different product. Buyers should verify the exact product, exact model, current labeling, and seller chain.
The phrase "FDA registered" is not enough. Registration and listing are administrative concepts. They do not, by themselves, mean a device has been authorized, cleared, or approved for a claimed medical use. A comparison page should never use another brand’s FDA status to imply the same status for Fitiger unless a product-specific record supports it.
|
Verification checkpoint |
Safer buyer interpretation |
|
Exact FDA status |
Check whether the exact product is authorized, cleared, only registered/listed, or unsupported for its claim. |
|
Second-line labeling |
The label should preserve first-line rescue first and second-line use only after unsuccessful standard measures. |
|
Seller traceability |
Authorized seller, batch, instructions, and replacement parts matter when copies or old claims circulate online. |
|
Performance claims |
Pressure, seal, and material claims should be tied to defined testing conditions. |
FoldPumpVac's folding format matters when it changes where the device can be staged. A device near the dining table, care cart, cafeteria station, travel bag, or vehicle kit has a different response geometry from a device kept in a distant cabinet.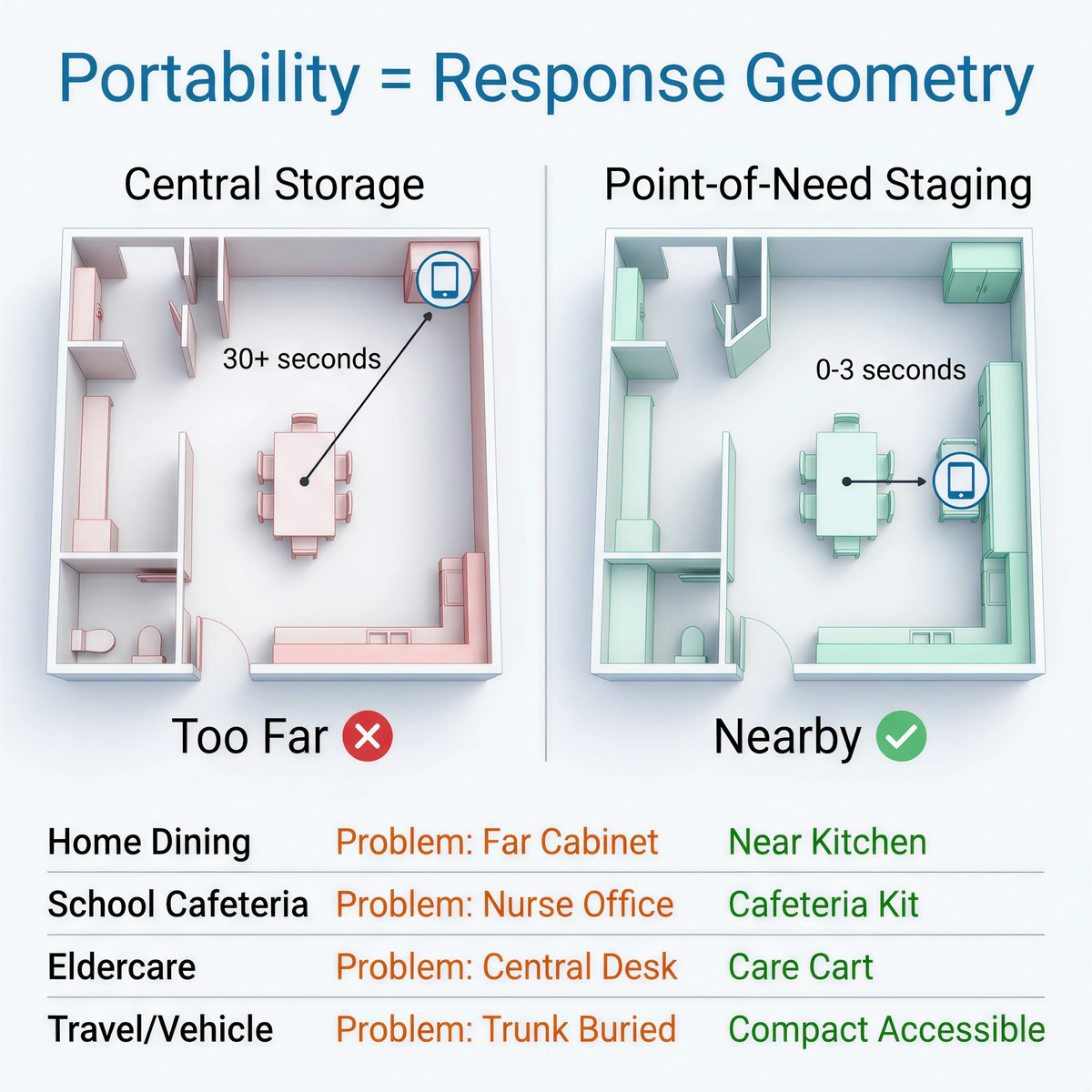
Point-of-need staging does not replace back blows, abdominal thrusts, chest thrusts, CPR readiness, 911, or EMS. It compresses one specific failure point: the time between deciding a second-line backup is needed and physically reaching it.
|
Setting |
Common retrieval problem |
FoldPumpVac placement logic |
|
Home dining |
The device is stored with general emergency supplies, far from meals. |
Stage near the kitchen or dining area in a visible, protected location. |
|
School cafeteria |
The nurse office or front office may be too far from lunch-period risk. |
Use cafeteria or event-kit staging inside the school response plan. |
|
Eldercare dining |
Residents eat in multiple rooms or shifts; staff movement is constrained. |
Place backup near dining rooms, care carts, or high-risk meal settings. |
|
Travel and vehicles |
A bulky device may get buried or left behind. |
Use compact staging where the caregiver can identify and reach it quickly. |
|
Daytime placement may not match after-dismissal room access. |
Plan distributed staging with role cards and retrieval paths. |
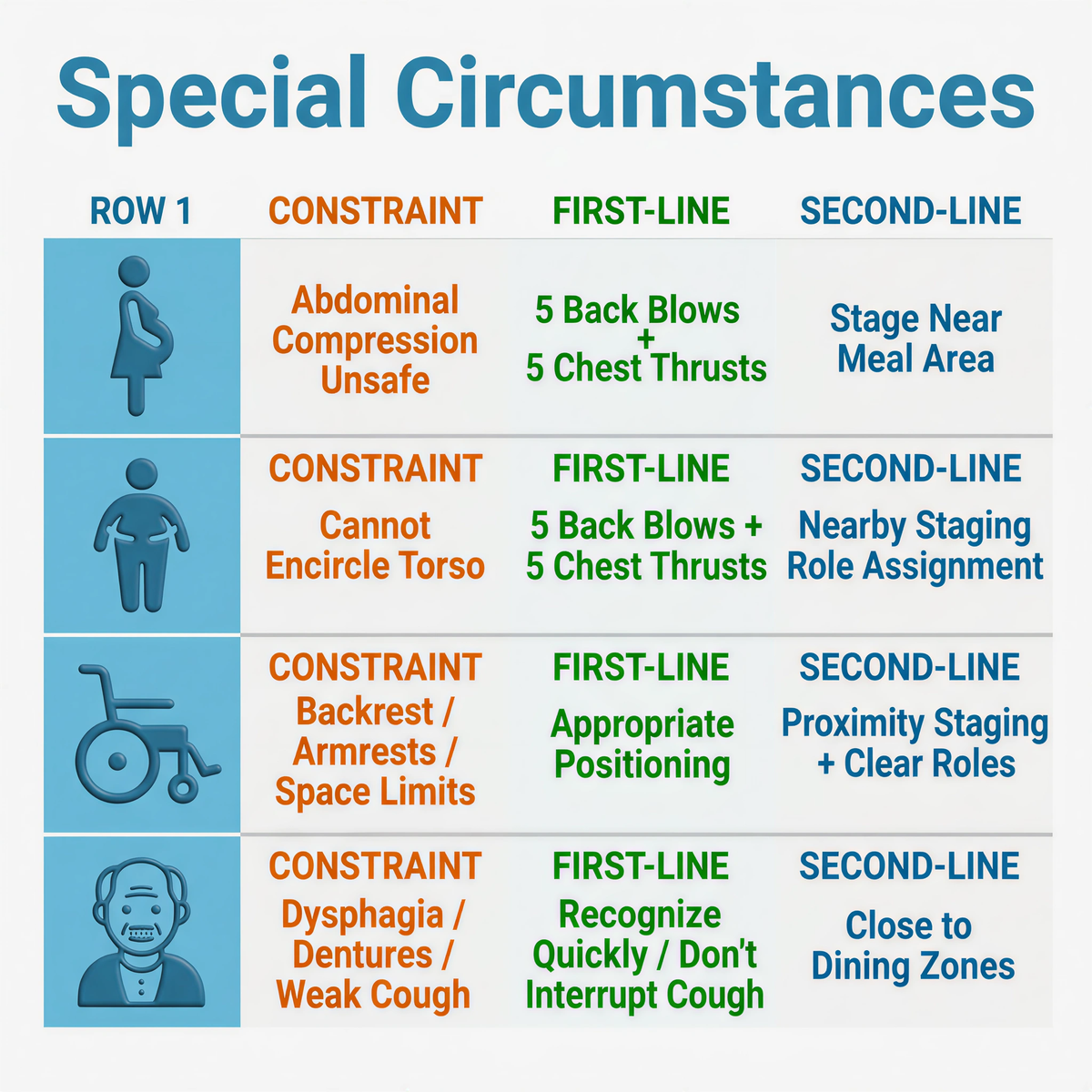
Manual rescue remains first-line. Some bodies and rooms make force delivery harder. Pregnancy shifts the force-generation point to the breastbone to avoid abdominal compression. Severe obesity can prevent a rescuer from encircling the torso or coupling force cleanly. Wheelchairs add backrests, armrests, trays, posture limits, and narrow room geometry.
The issue is not whether first-line rescue matters. It does. The issue is whether the plan has a second-line layer nearby if the first-line pathway cannot resolve the obstruction within the available oxygen window.
|
Special circumstance |
Physical constraint |
2025 first-line protocol emphasis |
Second-line redundancy judgment |
|
Late pregnancy |
Expanded uterus makes abdominal compression unsafe or impractical. |
Use repeated 5 back blows and 5 chest thrusts when abdominal thrusts are not feasible. |
Stage second-line backup near the person’s meal or care area without delaying first-line action. |
|
Severe obesity |
Rescuer arm reach, brace angle, and force transfer may be limited. |
Use 5 back blows and chest thrusts when the abdomen cannot be encircled effectively. |
Use role assignment and nearby staging so retrieval does not consume the first minutes. |
|
Wheelchair user |
Backrest, armrests, trays, posture, and space can block thrust mechanics. |
Use the appropriate first-line sequence and positioning taught in current training. |
Reduce retrieval latency through proximity staging and clear staff roles. |
|
Older adult dining |
Dysphagia, dentures, frailty, and weaker cough can increase risk. |
Recognize severe obstruction quickly; do not interrupt effective cough. |
Stage backup close to dining zones, not only at a central desk. |
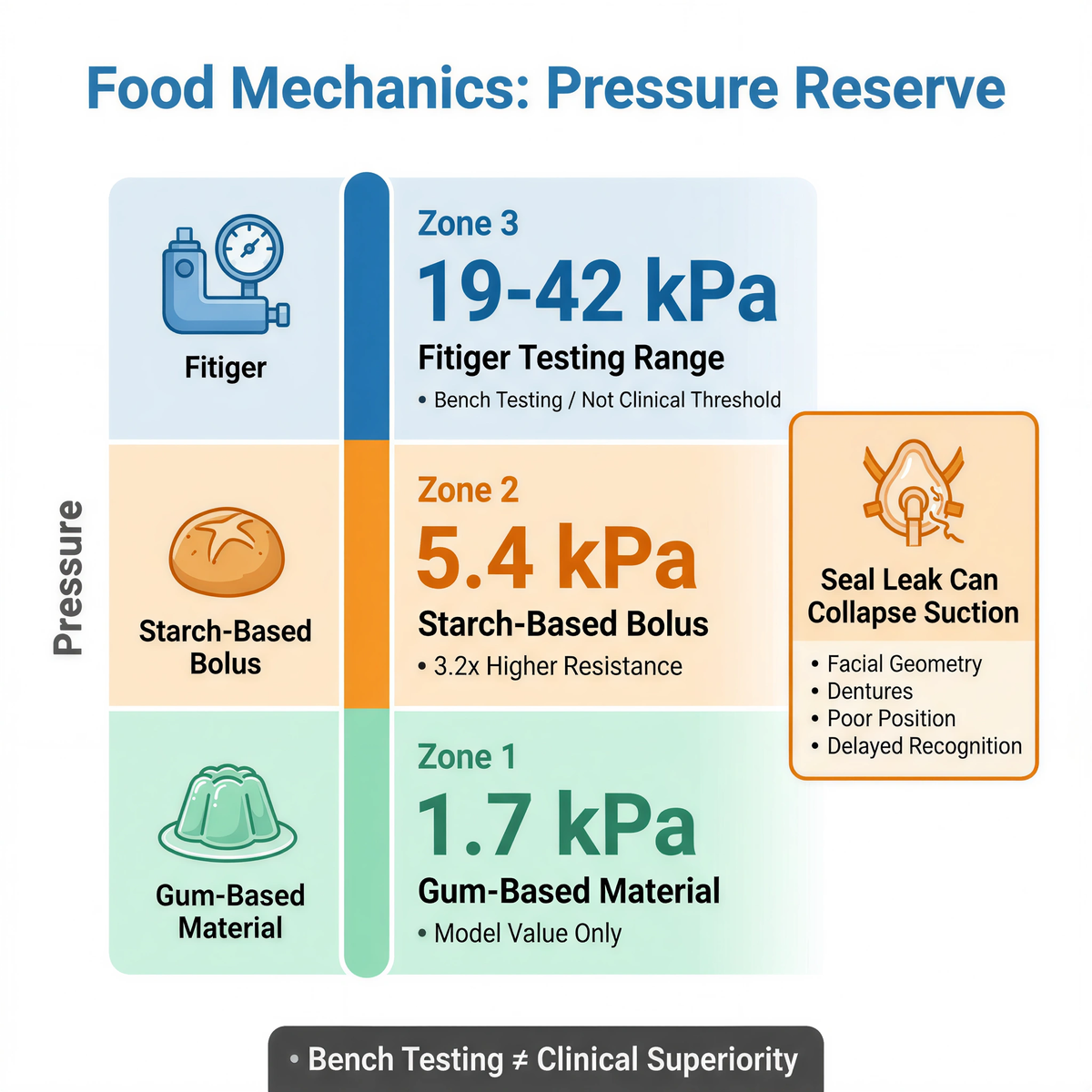
A choking event is a material problem before it becomes a product comparison. Food texture changes the force needed for displacement. Oral-flow simulator research has reported clearing-pressure examples near 5.4 kPa for starch-based material and about 1.7 kPa for gum-based material under tested conditions. That is about a 3.2-fold difference in model resistance.
Those values are not clinical thresholds for any suction device. They explain why generic “strong suction” language is weak. A second-line device needs measured mechanical reserve, and that reserve can be consumed by mask leak, facial geometry, dentures, poor positioning, or delayed recognition.
Fitiger evidence materials reference a 19 kPa to 42 kPa pressure/testing range. The useful claim is not guaranteed rescue. The useful claim is that FoldPumpVac can be discussed through defined test evidence rather than product photography alone.
|
Mechanics point |
Reader-friendly meaning |
Evidence boundary |
|
5.4 kPa starch-based bolus example |
Some solid food materials may resist movement far more than soft gel-like material. |
Model value only; not a clinical suction threshold. |
|
1.7 kPa gum-based material example |
Lower-resistance material may clear under less pressure in the model. |
Does not predict every real airway event. |
|
19 kPa to 42 kPa Fitiger testing range |
Fitiger can discuss pressure behavior with defined test context. |
Bench testing does not prove clinical superiority. |
|
Mask leak path |
A small edge lift can collapse useful suction during the pull phase. |
Seal inspection and mask condition remain essential. |
Suction depends on a pressure circuit: device body, valve behavior, mask geometry, face shape, user pull, and storage condition. The mask is often the weak link because it is the soft interface that has to adapt to human facial geometry.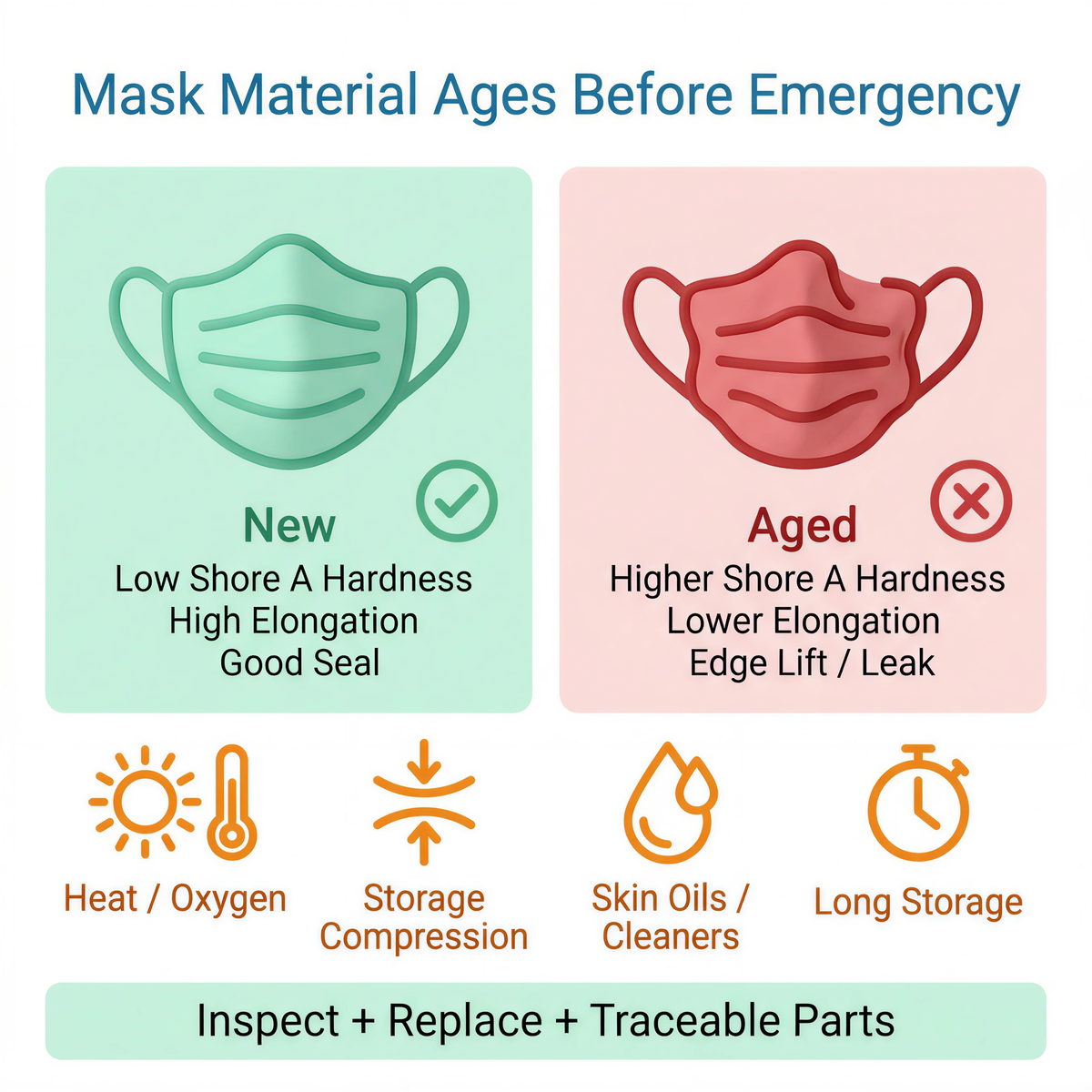
Medical-grade silicone can be appropriate for face-contact components, but silicone still has material aging behavior. Long storage, skin oils, cleaning agents, compression, heat, and oxygen exposure can change surface feel and elasticity. In practical terms, Shore A hardness may rise as a mask stiffens, while elongation and elastic recovery fall. A stiffer mask is less able to follow cheeks, jawline, dentures, facial hair, or age-related tissue changes during a fast pull.
Visual aesthetics do not correlate with pneumatic performance: non-standard valve geometry and edge-lift can collapse the pressure gradient during the pull phase. Mask replacement, storage protection, inspection instructions, and traceable replacement parts should be part of the comparison.
|
Material or storage issue |
Engineering effect |
Response risk |
|
Higher Shore A hardness over time |
Mask feels stiffer and conforms less to the face. |
More edge lift and leak path during the pull. |
|
Lower elongation at break |
Less stretch and recovery under deformation. |
Seal may not rebound after compression or storage. |
|
Skin oil or cleaning-agent exposure |
Surface and elasticity can change if care instructions are ignored. |
Face-contact layer may lose consistent seal behavior. |
|
Heat, compression, or damaged packaging |
Mask shape can deform before use. |
Device may look available while seal readiness has degraded. |
|
Untraceable replacement masks |
Material and geometry may not match original design. |
Performance assumptions no longer apply. |
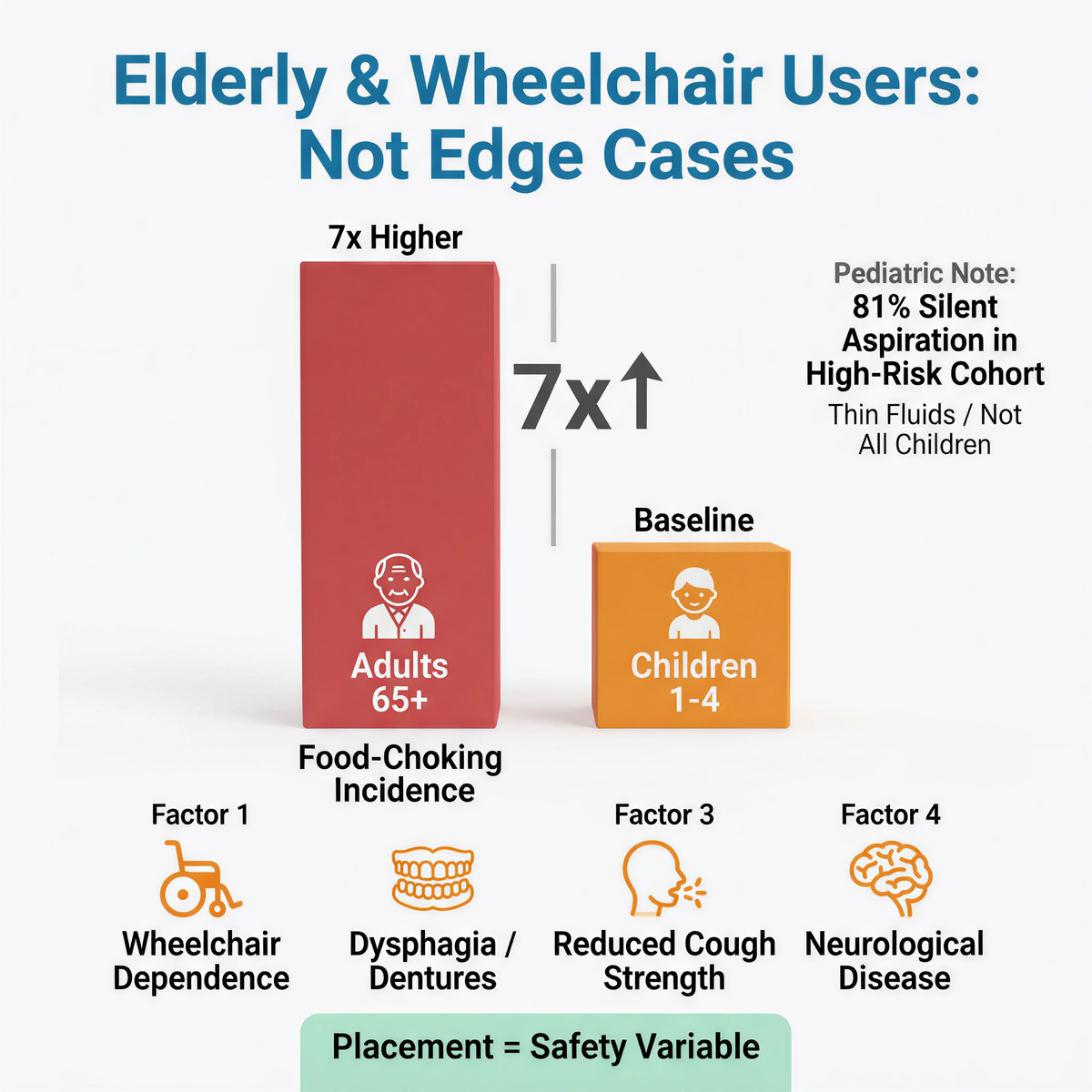
Food choking is often associated with children, but older adults are a major risk group. Geriatric swallowing literature reports that people older than 65 have a food-choking incidence seven times higher than children aged 1 to 4. Wheelchair dependence, frailty, dysphagia, dentures, neurological disease, and reduced cough strength turn “placement” into a safety variable, not a storage preference.
Pediatric swallowing evidence also shows why visible distress cannot be the only trigger. In one high-risk pediatric aspiration cohort, thin fluids were silently aspirated in 81% of aspirating patients. That number should not be generalized to all children or to foreign-body obstruction. Its relevance is narrower: some airway threats do not produce the loud, obvious signal that lay responders expect.
Rural and remote response conditions make device placement more important, but this article does not use unsupported EMS delay figures. The specific 97.1-minute versus 69-minute comparison was not included because no reliable public source was verified for that exact pair during fact-checking. A better-supported framing is still strong: peer-reviewed EMS response-time literature has reported average rural EMS arrival times above 14 minutes, with nearly 1 in 10 rural encounters waiting almost half an hour for EMS personnel.
|
Location context |
Supported latency concern |
Placement implication |
|
Urban home or apartment |
EMS may be faster, but building access and vertical response time can still add delay. |
Stage near the dining area and share location with household members. |
|
School or facility campus |
Internal retrieval, locked rooms, staff roles, and EMS entrance can add minutes. |
Use room-level staging and role assignment. |
|
Rural home or remote care site |
Published EMS literature reports longer rural arrival times, including averages above 14 minutes and high-delay outliers. |
Use vehicle, kitchen, and care-zone staging; do not rely on a single central storage point. |
|
Travel or road setting |
Exact location language and device access can be poor. |
Use compact kits and instructions kept with the device. |
LifeVac has strong public awareness and a public 2026 De Novo reference point. That awareness is valuable when buyers are new to the category. FoldPumpVac should not compete by pretending brand familiarity is irrelevant. It should compete where its design is most concrete: compact staging, retrieval geometry, material-contact discipline, and second-line response planning.
For a family, FoldPumpVac may be relevant when the device must live near the kitchen, dining room, grandparent’s room, or travel bag. For a school, it may be relevant when the cafeteria, after-school room, event kit, or bus zone is too far from a central cabinet. For eldercare, it may be relevant when dining rooms, room-level care, wheelchairs, and shift coverage create access gaps.
Do not assume LifeVac’s FDA status applies to every suction anti-choking device.
Do not assume Fitiger FoldPumpVac has the same product-specific FDA authorization unless a current product-specific record proves it.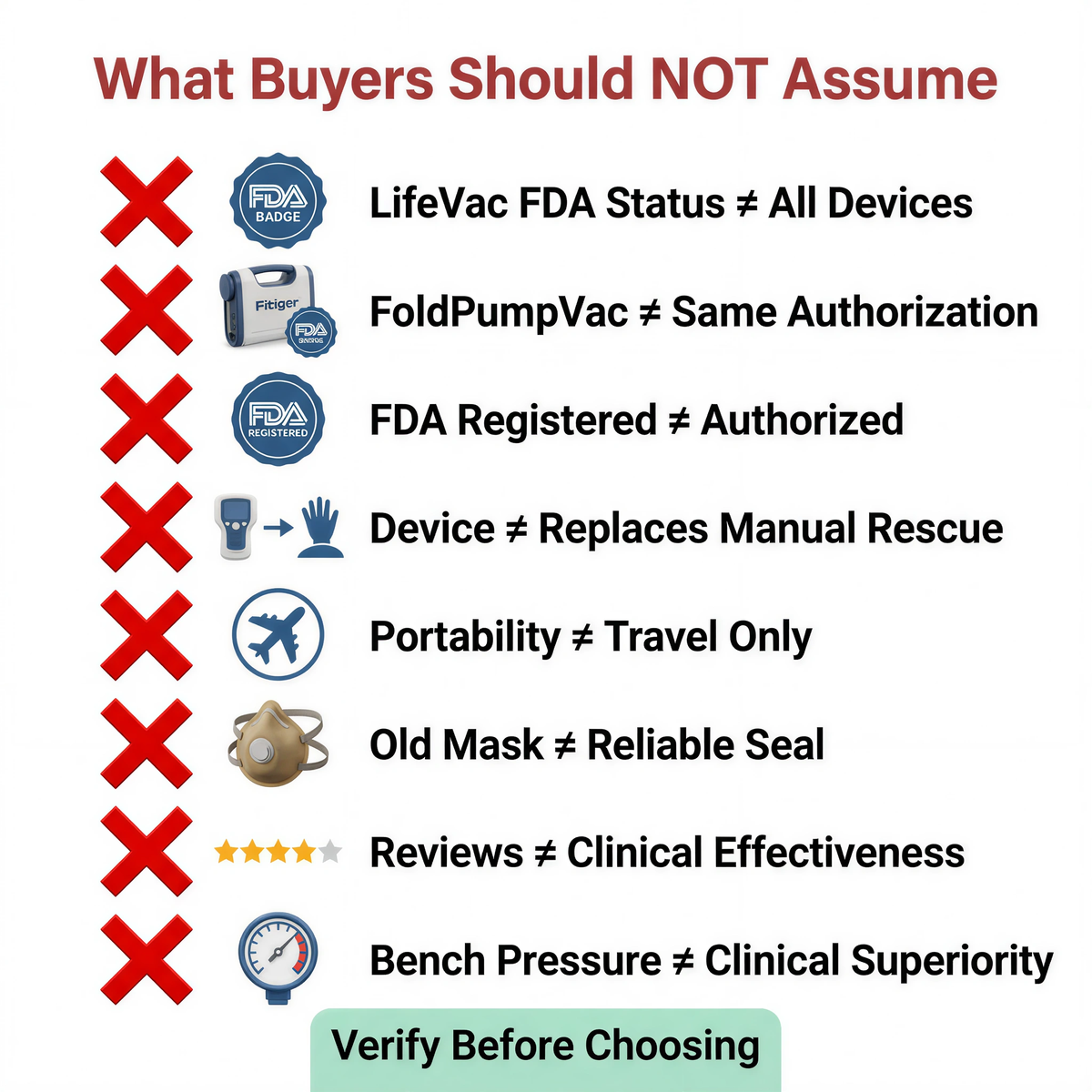
Do not assume "FDA registered" means product authorization.
Do not assume a second-line device replaces 5 back blows plus 5 abdominal thrusts, or chest thrusts when abdominal thrusts are the appropriate first-line alternative.
Do not assume portability matters only for travel.
Do not assume a mask seal is reliable if the mask is old, stiff, deformed, poorly stored, or replaced through an untraceable source.
Do not assume reviews prove clinical effectiveness.
Do not assume a bench pressure value proves clinical superiority.
Choose the response geometry before choosing the brand. Where will the device be staged? Who retrieves it? Can first-line rescue start without waiting for the device? Can the mask be inspected? Are replacement parts traceable? Does the product language preserve second-line use after unsuccessful standard measures? Does the evidence support the claim being made?
The stronger choice is the device that fits the response chain. In choking readiness, the room matters, the body matters, the mask matters, and time matters.
For campus-specific placement and readiness planning, review the school cafeteria.
Fitiger FoldPumpVac can be considered by buyers comparing second-line suction backup options. The comparison should focus on response sequence, exact product status, compact staging, seal design, material-contact evidence, storage readiness, and seller traceability rather than brand familiarity alone.
No. FoldPumpVac should not be described as a clinical replacement for LifeVac. It is a Fitiger second-line backup option with its own design approach, especially compact staging and portable readiness.
No. First-line choking rescue comes first. For most responsive adults and children with severe choking, the 2025 AHA sequence uses repeated cycles of 5 back blows and 5 abdominal thrusts. Chest thrusts are used when abdominal thrusts are not feasible. A suction device belongs later in the sequence after standard measures are unsuccessful.
Portability affects retrieval time. A device staged near kitchens, dining rooms, school cafeterias, care carts, travel bags, or vehicle kits may reduce distance from the emergency. It still does not replace manual rescue or emergency activation.
A mask seal depends on flexibility and shape recovery. If a silicone mask becomes stiffer, deformed, contaminated, or poorly stored, it may create leak paths during the pull phase. Inspection and replacement discipline matter.
No. Pressure testing helps describe mechanical behavior under defined conditions. It cannot prove clinical superiority in real airway emergencies, where food type, saliva, facial anatomy, positioning, timing, and user behavior all matter.
|
Source |
What it supports |
Full link |
|
FDA Safety Communication, March 4, 2026 |
Supports first-line choking rescue protocols first and anti-choking devices as a second option if standard measures are unsuccessful. |
|
|
FDA De Novo Order DEN250012 |
Supports 21 CFR 874.5400, product code QXN, and second-line suction anti-choking device classification. |
https://www.accessdata.fda.gov/cdrh_docs/pdf25/DEN250012.pdf |
|
American Heart Association 2025 Adult FBAO Algorithm |
Supports repeated cycles of 5 back blows and 5 abdominal thrusts for responsive adults with severe FBAO. |
|
|
American Heart Association 2025 Child FBAO Algorithm |
Supports repeated cycles of 5 back blows and 5 abdominal thrusts for responsive children with severe FBAO. |
|
|
Food Oral Processing and Tribology review |
Supports the 5.4 kPa versus 1.7 kPa oral-flow simulator comparison for different material behavior. |
|
|
Velayutham et al., Silent Aspiration: Who Is at Risk? |
Supports the pediatric silent aspiration data in a high-risk cohort and the need to avoid relying only on obvious cough signals. |
|
|
Cichero, Age-Related Changes to Eating and Swallowing Impact Frailty |
Supports geriatric choking risk discussion, including older-adult food-choking incidence compared with young children. |
|
|
Mell et al., Emergency Medical Services Response Times in Rural, Suburban, and Urban Areas |
Supports rural EMS latency discussion and the operational importance of proximity staging. |
This article compares public category information, buyer decision points, FoldPumpVac design intent, response sequence, portability, seal considerations, and Fitiger evidence boundaries. It does not prove clinical superiority over LifeVac. It does not replace first-aid training. It does not alter the first-line role of established choking rescue protocols. It does not imply product-specific FDA authorization unless that status is verified for the exact device.
Brand and evidence note
LifeVac is mentioned only for identification and comparison. LifeVac and other product names are trademarks of their respective owners. This article is an independent Fitiger buyer-education comparison based on public category information, response-sequence requirements, product-design considerations, and Fitiger evidence boundaries. It does not claim clinical superiority unless product-specific, comparable evidence directly supports that claim.
This article is for educational, engineering, and product-safety planning purposes only. It is not medical, legal, regulatory, or procurement advice. In a choking emergency, follow established first-line rescue protocols, call emergency services, and use any second-line device only within its authorized instructions and response sequence. Verify the FDA status of any exact product before making authorization, clearance, or approval claims.




















