Rural schools do not automatically need more emergency equipment than urban schools. They often need a different plan. Longer travel distances, limited nursing coverage, detached buildings, extended bus routes, smaller purchasing budgets, and fewer nearby backup resources can make access and response continuity harder to manage.
The central question is not how remote a school looks on a map. It is whether the school can start the correct response immediately, call for professional help, reach approved equipment, and maintain trained coverage across its actual operating hours.
Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions.
A rural school may be several miles from the nearest emergency department or ambulance base. That matters for planning, but it does not change the first actions staff should take during a choking emergency.
For a responsive person with severe airway obstruction, trained staff should activate emergency medical services and begin the applicable established choking first-aid procedure. If the person becomes unresponsive, CPR and dispatcher instructions become part of the response.
A suction-based anti-choking device belongs only in a second-line backup role after standard choking rescue has been attempted without success.
Longer EMS travel time does not justify delaying 911, skipping first-line care, or treating a device as a guaranteed substitute for trained rescue.
The school should plan for distance without allowing distance to distort the response sequence.
The term "rural school" can describe very different settings.
A small elementary school near a regional town may have a nearby volunteer ambulance service. A district campus in a mountain area may serve several communities and operate long bus routes. An agricultural school may have classrooms, workshops, athletic fields, and meal areas spread across a large property. A tribal, island, frontier, or remote community school may face transportation and communication conditions unlike those of a school only twenty miles away.
Planning should be based on the school's actual conditions, including:
| Road access | EMS coverage | Weather |
| Building layout | Enrollment | Staffing |
| Nurse availability | Radio and mobile coverage | Bus routes |
| After-school activities | Shared facilities | Local mutual-aid resources |
A rural label alone does not establish the risk or the solution.
Some rural districts share nursing staff across multiple schools.
A nurse may be present at one campus only on certain days or for part of the school day. Another employee may manage routine health needs when the nurse is elsewhere.
This creates several planning questions:
| Who leads the response when the nurse is off campus? | Which staff members hold current first-aid and CPR training? | Who checks emergency equipment? |
| Who can access health-office storage? | Who communicates with the nurse? | Who contacts EMS? |
| Who documents the event? | Who handles post-use equipment management? | Who speaks with families and district administrators? |
| The answer cannot simply be "call the nurse." |
The school needs an on-site response structure that works without assuming the nurse can arrive first.
Small enrollment does not always mean a compact campus.
A rural school may include:
| Main classroom building | Detached cafeteria | Agricultural workshop |
| Gym | Athletic field | Portable classrooms |
| Bus garage | Preschool building | Community-use hall |
| Vocational classrooms | Outdoor learning area |
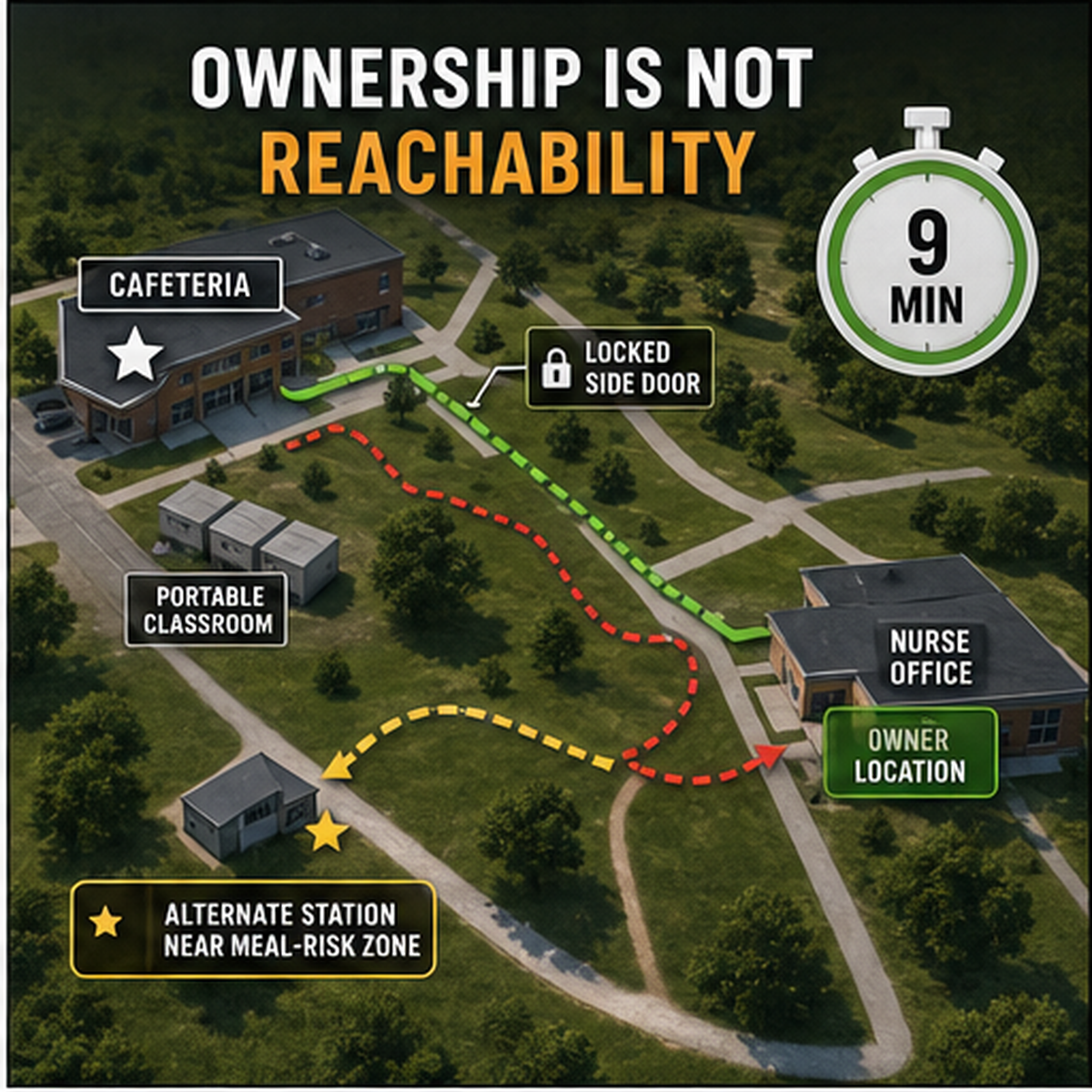
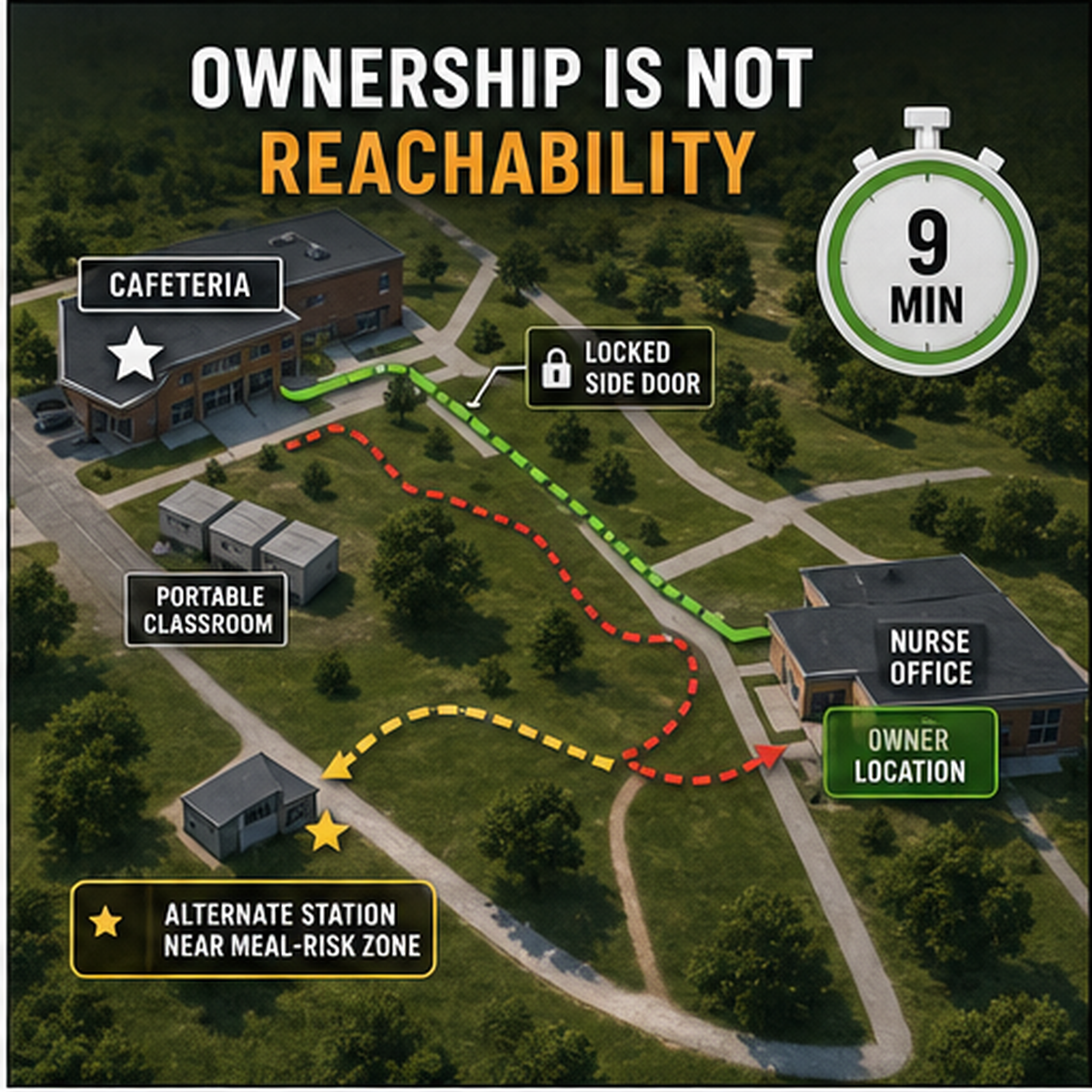
A single emergency cabinet in the main office may be technically central but operationally distant.
The school should walk the route from each occupied area and record:
| Door access | Distance | Stairs |
| Outdoor paths | Weather exposure | Keys or badges required |
| Staff familiarity | Radio coverage | Time away from the person needing help |
The goal is not to create a universal time limit. It is to identify avoidable delay.
In some rural areas, the route between buildings may be affected by:
| Snow | Ice | Heavy rain |
| Mud | Extreme heat | Wildfire smoke |
| Flooding | High winds | Limited lighting |
A placement that works during a clear fall afternoon may be difficult during a winter storm or evening event.
The school should review whether staff must cross outdoor space to reach emergency equipment and whether the route remains usable during seasonal conditions.
| Possible corrections may include: | Moving equipment inside the occupied building |
| Adding an approved secondary location | Improving exterior lighting |
| Assigning after-hours access | Keeping walkways clear |
| Updating winter inspection procedures | Reviewing portable storage for field activities |
Seasonal risk should be built into the access plan rather than treated as an unusual exception.
Some rural communities rely heavily on volunteer emergency medical responders or fire departments.
These responders may know the school well and provide valuable local support. Response availability may still vary by time, distance, staffing, road conditions, and simultaneous calls.
The school should coordinate with local responders where appropriate, but it must retain its own immediate responsibilities.
Useful coordination topics include:
| Preferred EMS entrance | Building labels | Gate access |
| Road conditions | Campus maps | Radio contact |
| Exact address wording | Bus route location reporting | Athletic field access |
| After-hours building use | Staff meeting responders |
A local responder's familiarity with the campus is helpful. It should not replace clear signs, accurate addresses, or trained school staff.
A school may be relatively close to EMS and still lose time because the call does not identify the correct location.
| Communication problems may include: | Weak mobile signal | Shared phone line |
| No radio in a detached building | Incorrect street address | Unmarked entrance |
| Locked gate | Several buildings with similar names | No one assigned to meet responders |
| Bus route without a precise location method |
Each occupied area should have a practical emergency communication method.
A posted location card may include:
| School name | Street address | Building |
| Room or area | Entrance | Gate code |
| Nearest road | Local landmark | Person assigned to meet EMS |
For buses, field trips, and athletic events, staff need a method for reporting a changing location.

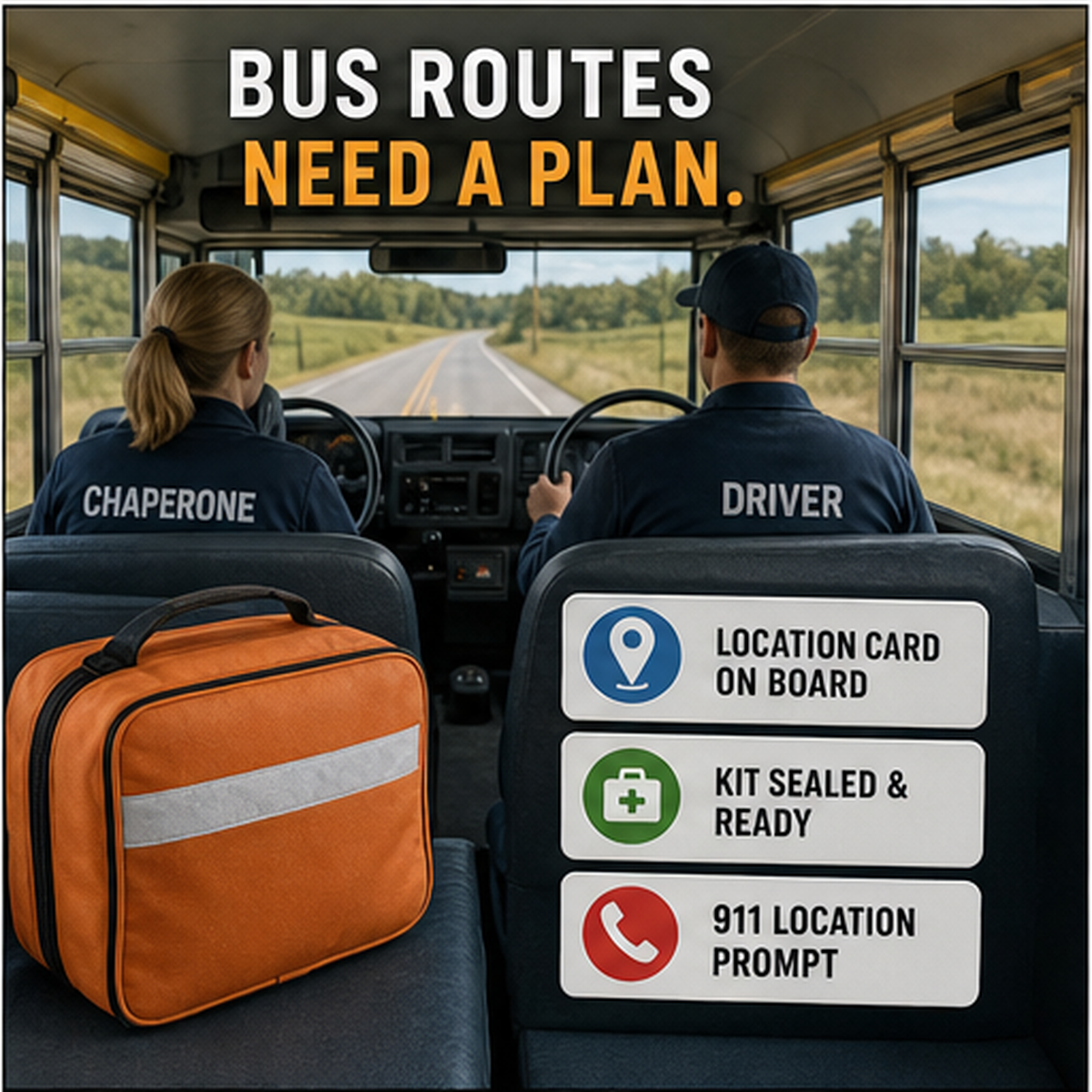
A student may spend an hour or more on a rural bus route.
The bus is not simply an extension of the school nurse's office. It is a mobile environment with limited space, changing locations, temperature exposure, traffic hazards, and potentially one adult responsible for the vehicle and every passenger.
A rural transportation review should address:
| Whether the bus has an attendant | Driver first-aid training | Communication with dispatch |
| Mobile or radio coverage | GPS or route-location information | Safe stopping procedures |
| Equipment storage | Temperature limits | Daily or scheduled inspection |
| Substitute buses | Vehicle reassignment | Student-specific transportation plans |
| Post-incident reporting | Replacement after use |
An emergency kit assigned to a bus needs a vehicle number, custodian, inspection owner, and transfer record.
It should not move between buses informally.
During an emergency, the driver may need to:
| Stop the vehicle safely | Secure the bus |
| Contact dispatch or 911 | Supervise other students |
| Identify the location | Begin or support first aid |
| Direct arriving responders |
A bus attendant can change the operating plan considerably.
Where no attendant is present, the district should define what the driver does first and how dispatch supports the response.
The plan should not assume that the driver can continue operating the vehicle while providing care.
It should also avoid placing equipment where it obstructs exits, interferes with driving controls, or becomes a loose object during transit.
A district may assign equipment to a regular bus and lose coverage when that vehicle is replaced for maintenance.
A transportation system should define:
| Whether equipment follows the route or the vehicle | Who transfers it |
| How the transfer is recorded | Who inspects the substitute bus |
| What happens if no replacement kit is available | How drivers are notified |
| How the route record is updated |
A label reading "Bus 12" is not useful when the route is temporarily operating on Bus 27.
The custody system must survive reassignment.
Many rural school buildings also serve as community centers.
Gyms, cafeterias, fields, auditoriums, and meeting rooms may remain active during:
| Evening sports | Weekend tournaments |
| Community dinners | Local meetings |
| Fundraisers | Agricultural events |
| Summer programs | Youth clubs |
The main office and health office may be closed during these events.
The school should identify:
| Event supervisor | Trained responders | 911 caller |
| Exact EMS entrance | Equipment access | Cabinet keys |
| Inspection owner | Post-event security | Incident reporting route |
A device available during school hours may be inaccessible during the event that draws the largest crowd.
A rural school may operate with a small team in which one employee holds several roles.
The principal may also manage transportation. A secretary may handle health-office access. A teacher may coach after school. The cafeteria manager may supervise community events.
This can make coordination efficient, but it can also create single points of failure.
Ask:
| What happens when that person is absent? | Who has the second key? |
| Who knows the location? | Who can order a replacement? |
| Who reviews inspection records? | Who manages the next shift? |
| Who takes over during a field trip? |
Every critical task should have a backup owner.
The program should remain functional during illness, leave, turnover, or severe weather.
Rural districts may face limited purchasing budgets and fewer grant-writing resources.
This can affect:
| Training frequency | Equipment quantity |
| Replacement stock | Communication systems |
| Cabinets | Signage |
| Transportation supplies | Staff coverage during training |
Budget limitations are real, but they should not lead the school to treat a donated device as a complete program.
The school still needs:
| Prevention | First-aid and CPR coverage |
| 911 access | Role assignments |
| Equipment management | Inspection |
| Documentation | Post-use procedures |
Funding should support the plan rather than substitute for one.
Some readiness gaps can be corrected without purchasing another device.
Examples include:
| Updating the emergency address card | Moving an existing cabinet | Removing an unnecessary lock |
| Providing a backup key | Improving signage | Adding equipment to substitute-staff orientation |
| Assigning a backup inspector | Updating bus transfer records | Correcting the campus map |
| Testing radio coverage | Clarifying who meets EMS |
These changes may produce more operational value than adding equipment to an unmanaged system.
A school should not use budget limitations as a reason to ignore low-cost access corrections.
A rural school donation request should connect each requested unit to a specific location or route.
For example:
Our district elementary school serves 310 students in three detached buildings. The cafeteria and gym are located across an outdoor walkway from the main office, and the nurse is on campus three days per week. We are requesting two choking emergency kits for approved staff-accessible locations in the cafeteria and gym. The cafeteria manager and athletic director will serve as primary owners, with the principal's designee as backup.
A transportation request may state:
The district operates two rural routes exceeding 45 minutes each. We are requesting one secured kit for each assigned bus, subject to district approval. The transportation director will manage inspection, transfer records, temperature review, and substitute-bus procedures.
These statements describe a manageable operational need.
They do not promise a clinical outcome.
A rural application should not say:
EMS will never arrive in time.
Rural students are less safe than urban students.
The device guarantees survival.
Every bus legally requires this product.
One donation will make the district compliant.
The product eliminates the need for training.
The school has no other emergency response.
Such claims may be inaccurate and can weaken credibility.
A better application describes distance, coverage, staffing, location, and access without turning uncertainty into certainty.
A school with 150 students may have a greater equipment-access problem than a school with 1,000 students if it operates across multiple buildings, routes, or remote activity areas.
The need assessment should consider:
| Number of locations | Travel paths | Operating hours |
| Staffing | Communication | EMS access |
| Bus routes | Existing equipment | Inspection capacity |
| Seasonal conditions |
Enrollment is one factor, not the entire formula.
A rural school map may need to show:
| Main campus | Detached buildings | Bus routes |
| Athletic fields | Agricultural areas | Vocational shops |
| Community-use buildings | EMS entrances | Gates |
| Unpaved roads | Radio dead zones | Equipment locations |
| Winter access routes | Alternate entrances | Nearby responder stations |
The map should be useful to staff, dispatchers, and administrators.
It should not rely on local nicknames that an outside responder may not recognize.
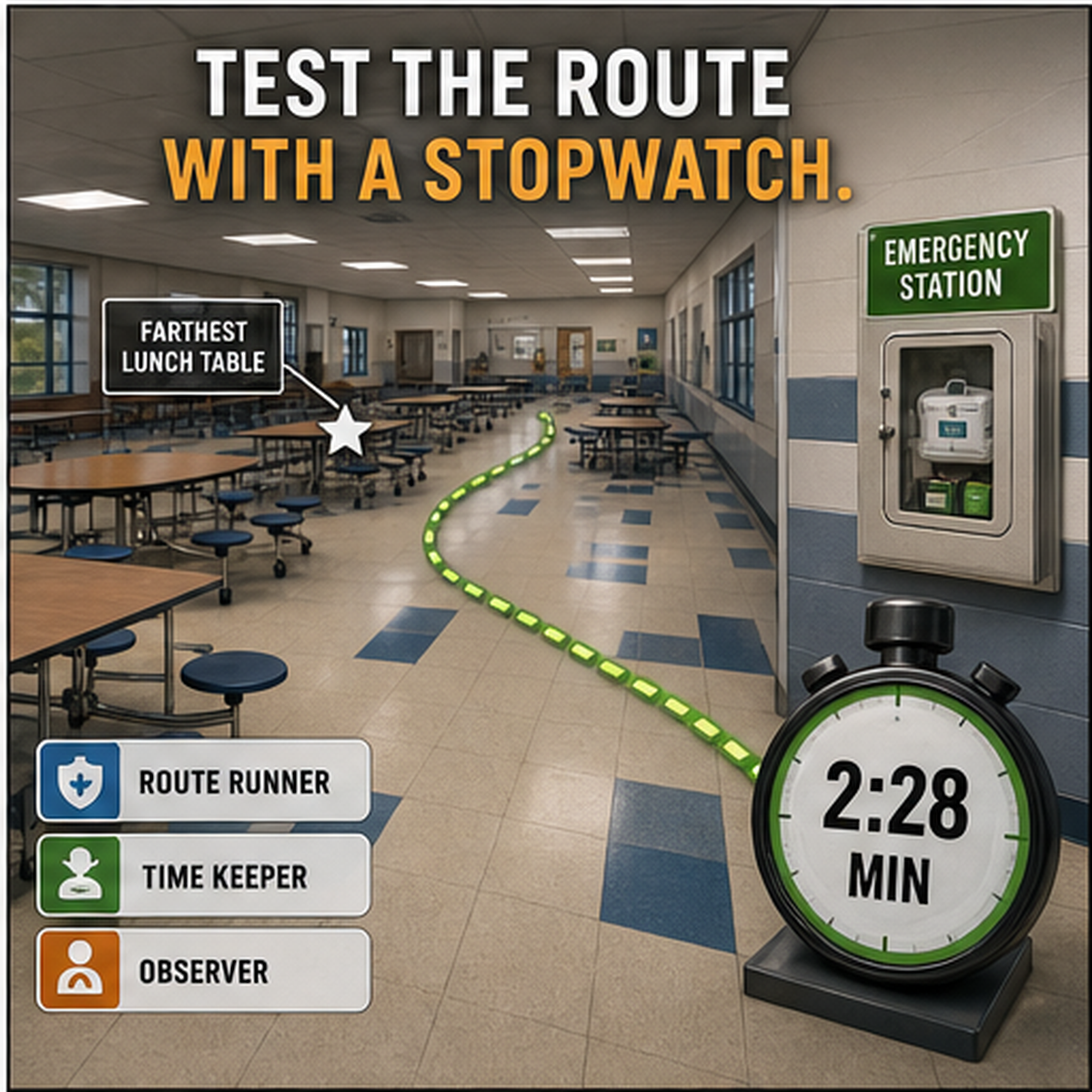
Do not test access only on a quiet morning with every door open.
A realistic audit may occur during:
| Lunch service | Evening athletics |
| Winter weather | Substitute staffing |
| Bus loading | Community use |
| Nurse absence | Weekend event |
The purpose is not to create drama.
It is to determine whether the plan survives ordinary variation.
Record:
| Who responded | Who called |
| Which route was used | What access failed |
| Whether the location was clear | Whether the kit was complete |
| What corrective action followed |
A plan that works only under ideal conditions is not dependable.
A small rural school may not control every relevant decision.
The district may manage:
| Procurement | Transportation | Insurance |
| Legal review | Training | Equipment standards |
| Record retention | Nursing | Building access |
| Donations | Incident reporting |
A building-level project should identify which decisions require district approval.
This prevents a school from accepting equipment that cannot be placed, maintained, or incorporated into district procedures.
A donation may be appropriate when the school has identified a real access or coverage gap and can manage the equipment responsibly.
Before applying, the school should be able to state:
| School and district identity | Location and service area | Existing equipment |
| Uncovered building or route | Requested quantity | Proposed placement |
| People served | Primary owner | Backup owner |
| Inspection plan | Training status | Shipping contact |
| Non-resale commitment |
Rural schools with a documented placement or transportation gap can review equipment donation support for rural schools through the FITIGER Donation Program.
Submitting a request does not guarantee approval, quantity, training, shipping, international delivery, or delivery by a requested date.
Staff can recognize severe airway obstruction.
Trained first-line responders are available.
911 can be activated without delay.
CPR readiness is documented.
Second-line equipment does not replace first-line rescue.
The response plan works when the nurse is absent.
On-site staff roles are defined.
Health-office access is not dependent on one person.
A backup owner is named.
Detached facilities have been reviewed.
Outdoor routes remain usable seasonally.
Locked doors and gates have backup access.
Evening and weekend use is covered.
Each area has a working call method.
Exact location wording is available.
Radio and mobile dead zones are known.
Someone is assigned to meet responders.
Drivers and attendants know their roles.
Equipment is assigned and secured.
Substitute-bus transfers are documented.
Route location can be reported accurately.
Temperature exposure is reviewed.
Each location has a primary and backup owner.
Inspection records are current.
Missing components trigger corrective action.
Post-use quarantine and replacement are defined.
Donation status is recorded accurately.
Funding
Low-cost access corrections are addressed first.
Remaining equipment needs are location-specific.
Long-term replacement costs are considered.
Donation requests are not used as a substitute for planning.
A rural preparedness program should avoid two opposite errors.
The first is assuming distance makes meaningful planning impossible.
The second is assuming one donated device solves the problem created by distance.
Neither is accurate.
Rural schools can strengthen readiness by making communication, role ownership, access, transportation procedures, and equipment management more explicit.
Those systems matter whether EMS is five minutes away or fifty.

Use donation support for defined gaps
For related planning context, review the anti-choking device buyer evidence checklist.
Not automatically. Need depends on building layout, travel distance between occupied areas, bus routes, staffing, after-hours programs, communication, existing equipment, and the school's ability to manage each location.
Rural schools may face longer EMS travel, shared nursing staff, detached buildings, long bus routes, weaker mobile coverage, seasonal access problems, and fewer nearby backup resources. These conditions require more explicit planning but do not change the first-line response sequence.
Yes. The application should explain nursing coverage and identify which on-site staff will manage first aid, equipment inspection, communication, and post-use procedures when the nurse is absent.
Not automatically. The district should review route length, staffing, storage, temperature exposure, communication, inspection, substitute buses, product labeling, and local policy before deciding.
Yes, when each requested unit corresponds to a documented building, route, or access gap. Approval may be for fewer units than requested.
No. Staff should call 911 and begin established first-line choking rescue. A suction-based anti-choking device belongs only in a second-line role after unsuccessful standard rescue.
The district should identify alternative communication methods, such as landlines, radios, dispatch procedures, or other approved systems, and test them in the areas where students and staff are present.
Only when the office provides reliable access for the locations and hours being covered. Detached cafeterias, gyms, buses, and evening programs may need separate review.
That depends on the specific donation program. Product donation should not be assumed to include certified first-aid or CPR training unless the program explicitly provides it.
No. Equipment alone does not establish compliance. The district must review applicable laws, policies, training, procurement, storage, inspection, documentation, and product instructions.
FITIGER Donation Program - Supports the donation planning pathway for rural schools with documented equipment gaps.
American Red Cross Adult and Child Choking First Aid - Supports established first-line choking response education.
U.S. Food and Drug Administration, 2026 Safety Communication - Supports standard rescue first and second-line device boundaries.
This article is for general education, rural school planning, and emergency preparedness. It is not medical advice, legal advice, a required equipment standard, or a substitute for certified first-aid training, manufacturer instructions, district policy, or professional review.




















