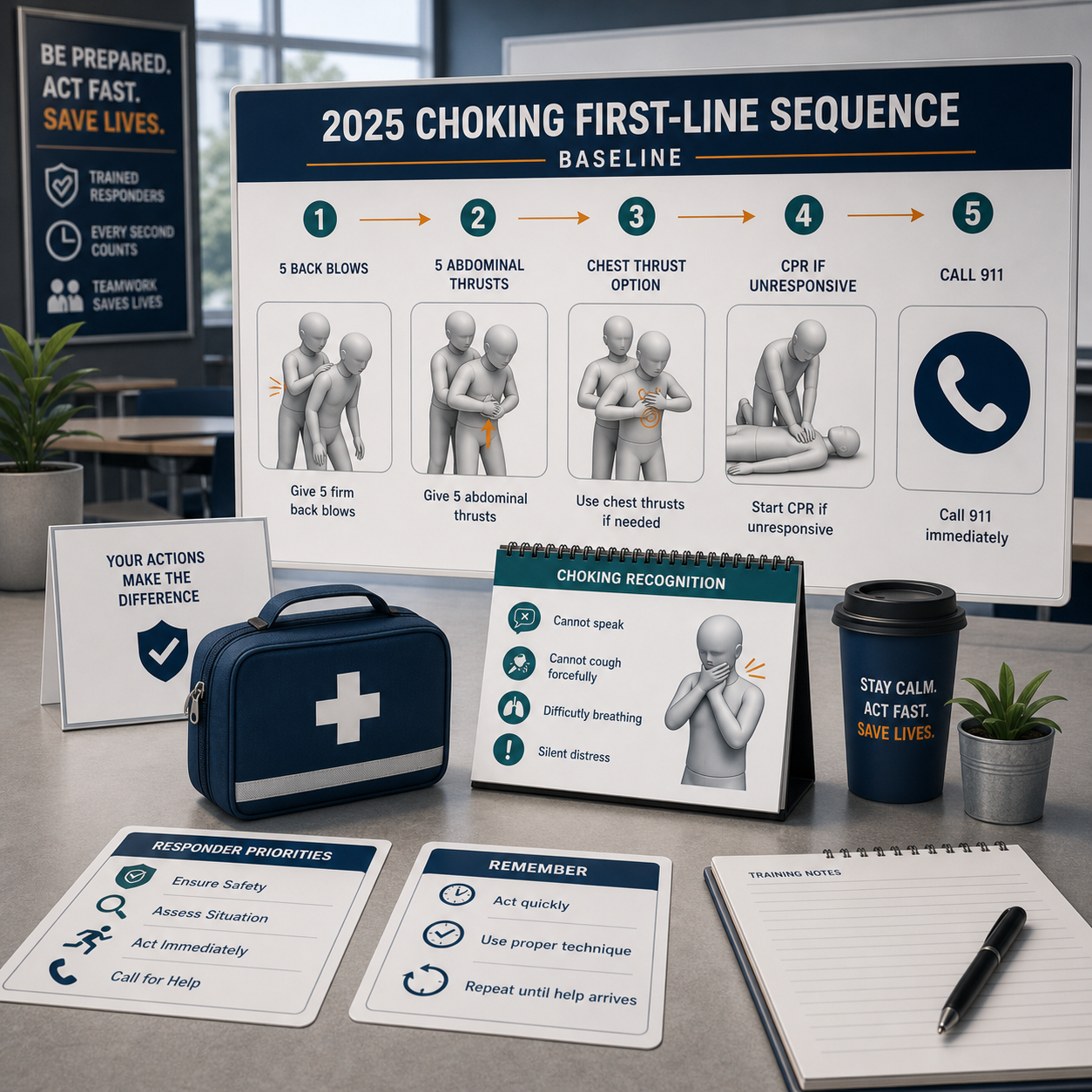
Choking rescue has physical limits in pregnancy, severe obesity, and wheelchair use. The 2025 AHA baseline is 5 back blows plus 5 abdominal thrusts for most conscious adults and children over 1; use chest thrusts instead of abdominal thrusts when abdominal access is unsafe or ineffective. QXN suction devices remain second-line after manual protocol fails. For a household checklist, see Fitiger's child and home choking safety readiness plan. Before choosing equipment, review Fitiger's anti-choking device buyer evidence checklist for FDA wording, testing, seller traceability, and kit-selection questions. |
The phrase Heimlich maneuver is still widely used, but it no longer describes the full current first-aid baseline. The 2025 AHA update places conscious adult and child choking response into repeated cycles of 5 back blows followed by 5 abdominal thrusts until the object clears or the person becomes unresponsive. For infants, the sequence is 5 back blows followed by 5 chest thrusts; abdominal thrusts are not recommended for infants.
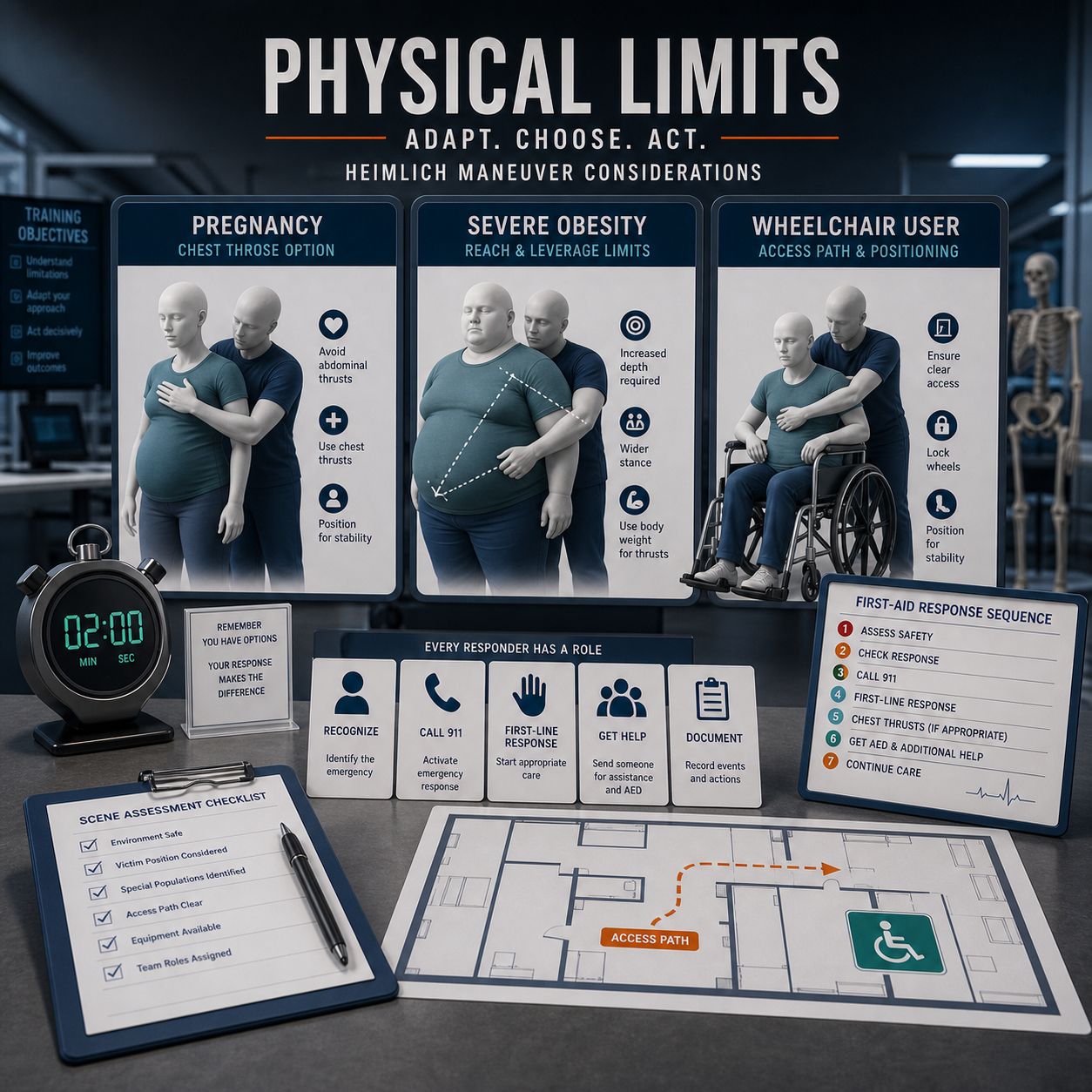
Real emergencies do not unfold inside a clean diagram. The rescuer may be smaller than the person choking. The torso may be blocked by a wheelchair backrest. Late pregnancy can make abdominal pressure unsafe. Severe obesity can prevent the rescuer from reaching the correct contact point. The protocol may be correct, yet the force path can still fail.
This article focuses on that gap: not whether first-line rescue matters, but whether the body, chair, room, and rescuer can physically deliver it fast enough inside the oxygen window.
For conscious adults and children over 1 with severe foreign-body airway obstruction, current AHA communication describes alternating 5 back blows and 5 abdominal thrusts. Medical references and first-aid instructions also specify chest thrusts for pregnant or obese people when abdominal thrusts cannot be performed safely or effectively. The operating question is no longer, "Can someone do the Heimlich?" It is, "Can this responder deliver the right 5+5 sequence on this body, in this position, right now?"
Person or scenario | 2025 first-line action | Critical boundary |
Conscious adult or child over 1 | Alternate 5 back blows and 5 abdominal thrusts. Continue until the object clears or the person becomes unresponsive. | Do not delay action while waiting for a preferred rescuer if a trained adult is present. |
Late pregnancy | Use 5 back blows and 5 chest thrusts when abdominal thrusts are unsafe or ineffective. | The pressure target moves away from the abdomen to reduce fetal and uterine risk while preserving thoracic pressure generation. |
Severe obesity | Use 5 back blows and chest thrusts if the rescuer cannot reach or anchor safely for abdominal thrusts. | Poor reach and unstable contact reduce force transfer before the first attempt begins. |
Infant under 1 | Alternate 5 back blows and 5 chest thrusts. | Abdominal thrusts are not recommended for infants. |
Unresponsive victim | Lower to a firm surface, activate EMS, begin CPR, and remove only a visible object when opening the airway. | Do not perform blind finger sweeps. |

Late pregnancy changes the available pressure path. The abdomen is no longer a neutral compression point, and the gravid uterus changes what the rescuer can safely target. Anatomical shifts redefine the rescue zone: pregnancy moves force generation to the breastbone when abdominal thrusts are unsafe, preserving a pressure-generating maneuver while avoiding direct abdominal compression.
A pregnant person can still experience a complete airway obstruction. The difference is that the rescue plan needs to be trained before the event. Staff should know where the hands go, how far to lean the person forward for back blows, and when to switch from abdominal to chest thrusts without debate.

Severe obesity creates a different failure mode. A rescuer may not be able to encircle the abdomen. The hands may land too far to the side, too high, too low, or on tissue that absorbs force instead of transmitting it cleanly. The movement can look correct while the effective displacement inside the airway remains inadequate.
That gap is one reason simple success comparisons can mislead safety teams. A first-line technique can remain correct in principle while losing efficiency in a real body. Training should cover chest thrust alternatives, kneeling position, two-responder support, and early EMS delegation rather than assuming one rescuer can always generate the necessary force.

Wheelchair choking response fails first at the access layer. A rigid backrest blocks rear positioning. Armrests, belts, side supports, footrests, seat angle, and limited transfer options narrow the working path. If the person cannot stand and transfer is not possible in seconds, the rescuer is no longer operating in the classic rear-standing geometry.
Training has to include the chair, not just the body. Facilities should rehearse front and side access, safe forward lean for back blows, whether the armrests can move, where the brakes lock, and who clears space around the chair. The named maneuver is less useful than a rehearsed access plan.
The strongest readiness plans separate medical priority from mechanical feasibility. First-line rescue stays first. The next question is whether the rescuer can physically deliver the correct maneuver on the person in front of them.
Scenario | Physical constraint | 2025 AHA first-line protocol | Engineering redundancy |
Late pregnancy | Uterine displacement and unsafe abdominal compression path. | 5 back blows + 5 chest thrusts when abdominal thrusts are unsafe or ineffective. | QXN suction device as second-line backup after unsuccessful BLS choking protocol, if allowed by policy and labeling. |
Severe obesity | Increased girth, reach failure, leverage loss, and unstable hand placement. | 5 back blows + 5 chest thrusts when abdominal thrusts cannot be performed safely or effectively. | Redundancy becomes more important when manual force transfer cannot reach the necessary operating effect. |
Wheelchair user | Fixed backrest, armrests, belts, side supports, and limited transfer path. | 5 back blows + 5 abdominal thrusts when feasible; modify position, kneel, or use trained alternatives according to protocol. | Stage backup near eating areas to reduce reach latency after manual failure. |
Smaller caregiver, larger adult | Body-size mismatch reduces encircling, anchor stability, and upward force path. | Use the current 5+5 sequence with position adaptation and rapid second-responder callout. | Escalation plan must not depend on one rescuer overpowering an unfavorable geometry. |
Choking is biological, but rescue is also mechanical. During Fitiger engineering review of food-bolus mechanics, published and bench-model references were used to compare how different bolus types resist clearing forces. Starch-based solid food boluses may require about 5.4 kPa of clearing pressure in the referenced model, compared with about 1.7 kPa for more gelatinous material. Those values should not be read as a universal human threshold. They are useful because they show why obstruction type, body position, and pressure transfer all matter.
A pretzel, dense bread, meat, sticky rice, or compressed starch mass is not the same problem as a soft gel. If the rescuer cannot generate stable inward and upward force because of pregnancy, severe obesity, wheelchair hardware, or body-size mismatch, the manual sequence may reach its physical limit before the oxygen window closes.
FDA created the U.S. device type for suction anti-choking devices under 21 CFR 874.5400 and product code QXN. The De Novo order for DEN250012 defines this category as a second-line treatment used after unsuccessful use of a basic life support choking protocol in a complete airway obstruction emergency.
For institutions, that language is a boundary, not a marketing shortcut. A QXN suction device does not replace prevention, staff training, the 2025 first-line sequence, 911 activation, CPR readiness, or medical follow-up. It belongs in the failure pathway: the moment manual protocol has not cleared the obstruction and a trained person can use the device without delaying BLS actions.
Layer | Primary purpose | Operational test |
Prevention | Reduce the chance of choking before the meal or activity begins. | Are high-risk foods, dysphagia plans, supervision needs, and seating conditions controlled? |
First-line manual rescue | Move air and pressure through the torso using current choking guidance. | Can the nearest responder perform the correct 5+5 sequence on this body in this position? |
Second-line QXN backup | Provide suction-based redundancy after unsuccessful BLS choking protocol. | Is the device policy-authorized, labeled for the situation, reachable in seconds, and assigned to a trained responder? |
EMS and CPR readiness | Manage deterioration and residual risk. | Who calls 911, who starts CPR if unresponsive, who meets EMS, and who documents the event? |
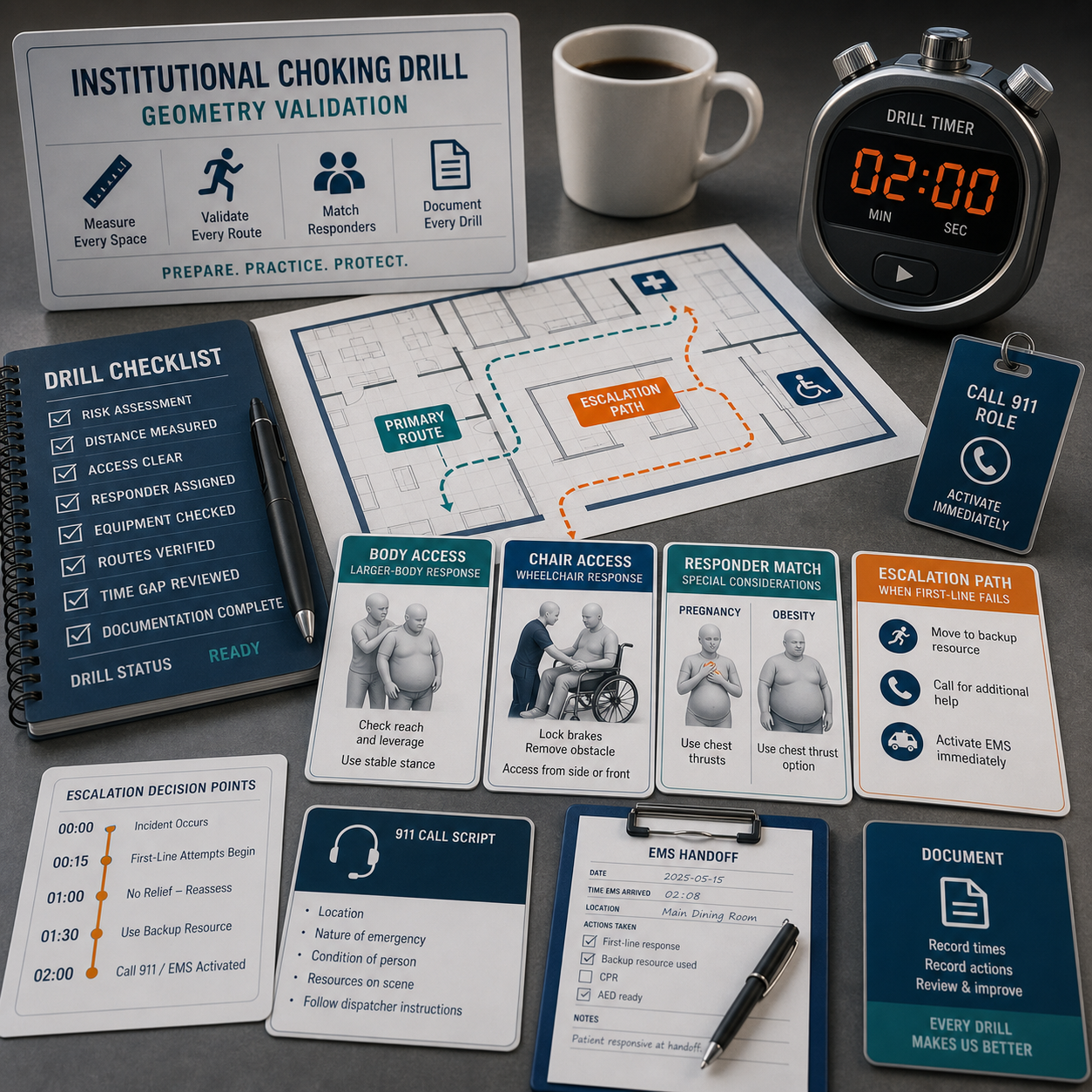
A serious choking drill should not stop at the correct hand motion. It should test the geometry that will exist on the floor, in the dining room, on the bus, beside the wheelchair, or in the family kitchen.
Validation point | Question to test | Failure sign |
Body access | Can the first responder reach the correct thrust point or chest-thrust position? | Responder cannot encircle, stabilize, kneel, or reach because of body size, pregnancy, or seating. |
Chair and room access | Can the wheelchair brakes lock, armrest move, torso lean forward, and space clear within seconds? | The first minute is spent moving furniture, arguing about transfer, or searching for a stronger rescuer. |
Responder match | Is the likely first responder physically able to deliver the trained sequence? | The plan depends on a staff member who may not be present during meals or transport. |
Escalation path | What happens after failed manual attempts? | No one calls 911, brings backup, starts CPR readiness, or retrieves a policy-authorized device. |
Post-event review | Does every severe choking event create a record and design fix? | The event closes as a story instead of producing a change to placement, staffing, food control, or training. |
The better question is whether the rescue system can convert knowledge into force under the conditions that actually exist. Pregnancy changes the safe pressure zone. Severe obesity changes reach and leverage. Wheelchair use changes access. Body-size mismatch changes force transfer. Dense food changes the clearing demand.
The engineering conclusion is direct: airway preparedness must validate the rescue geometry before the event. If first-line rescue is physically constrained, the plan needs trained alternatives, fast EMS activation, CPR readiness, and a defined second-line pathway that does not delay manual care.
The term is still widely used, but the current adult and child choking baseline is broader than abdominal thrusts alone. For conscious adults and children over 1 with severe choking, current AHA communication describes alternating 5 back blows and 5 abdominal thrusts until the object clears or the person becomes unresponsive.
Use 5 back blows and chest thrusts when abdominal thrusts are unsafe or ineffective. The pressure target moves to the breastbone because late pregnancy changes the abdominal risk zone. Call 911 immediately when severe choking is suspected.
Begin with the current first-line sequence, but use chest thrusts instead of abdominal thrusts when the rescuer cannot safely reach or anchor around the abdomen. Severe obesity can reduce leverage and force transfer, so early delegation, EMS activation, and backup planning matter.
No. QXN suction anti-choking devices are second-line devices under the FDA framework. They may be used only after unsuccessful BLS choking protocol in a complete airway obstruction emergency, according to device labeling, training, and local policy.
They should include the actual chair and room setup. Test backrest access, armrests, brakes, belts, forward lean, side access, and who clears space. A drill that only practices standing abdominal thrusts does not validate wheelchair rescue readiness.
Pressure values help explain the mechanical side of choking rescue. They should not be treated as a universal clinical threshold. They show that different food boluses can require different clearing forces and that poor body access can reduce the effectiveness of manual rescue.
American Heart Association Newsroom - Supports the 2025 choking update: 5 back blows followed by 5 abdominal thrusts for conscious children and adults, and 5 back blows plus 5 chest thrusts for infants. URL
AHA Adult Basic Life Support Guideline, 2025 - Supports the adult BLS choking recommendation and the rationale for alternating back blows and abdominal thrusts. URL
MedlinePlus Medical Encyclopedia - Supports the practical instruction that pregnant or obese people should receive chest thrusts instead of abdominal thrusts. URL
American Red Cross Adult and Child Choking First Aid - Supports public first-aid training language for 5 back blows and 5 abdominal thrusts and CPR transition if unresponsive. URL
FDA De Novo DEN250012 - Supports FDA Class II classification of suction anti-choking device as a second-line treatment after unsuccessful BLS choking protocol. URL
FDA Product Code QXN TPLC Page - Supports product code QXN, regulation number 874.5400, device class 2, and second-line intended-use wording. URL
This article is for emergency preparedness planning and educational support. It is not medical advice, diagnosis, treatment, or a replacement for hands-on CPR or first-aid training, EMS/911 activation, device labeling, or local policy. In an emergency, call 911 and follow dispatcher instructions. Institutions should train to current AHA, Red Cross, local EMS, and policy requirements before deploying any second-line device.




















